

National Cancer Institute
Predictably, the GOP has capitalized on the recent uproar over revised mammogram recommendations as proof that the federal government is trying to ration your health care. And while the US Preventive Services Task Force (the panel doing the recommending) consists of 16 doctors who review the research and conduct risk-benefit analysis—the GOP is more or less correct. The government is trying to ration health care. And it should, according to Princeton University bioethicist Peter Singer.
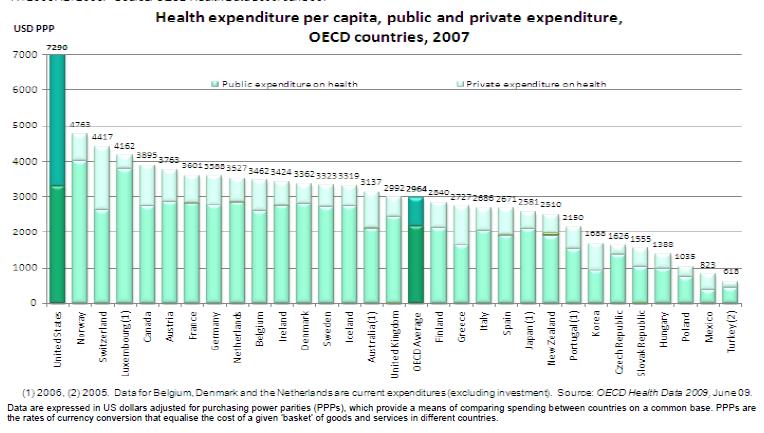
I’m with Singer. In seeking the status quo, do these pols really imagine that health care isn’t now rationed by private insurers? Of course not. They’re just grandstanding. Fact is, no medical rationing is more extreme than kicking someone out of your health plan. Costs do need to be controlled, for sure, but the costs are just a symptom of bad decisions and perverse incentives that have made America’s health care system No. 37 in the world—even though we’re No. 1 in per-capita spending. A lot of those bad decisions involve unnecessary testing, followed by treatment for conditions that are not, in the end, life-threatening. I’m not talking about withholding a lifesaving treatment from your 75-year-old mother here, but rather about approaching health—and mortality—with rational medicine rather than emotional politics.
We could get into the whole debate about death with dignity, but let’s not. Instead, consider this: Would you pay out of pocket to be screened for a condition you are very unlikely to have, and which would require invasive followup if you test positive? If yes, then why this particular condition—why not get tested for every condition for which a test exists? If your answer is no, you wouldn’t pay for it yourself, then why should anybody else? Why should your insurer?
In the specific case of mammograms as a way to detect breast cancer, the advisory panel recommended delaying routine tests until age 50—previously, it was 40—and doing those tests every other year rather than annually. Mother Jones, incidentally, made a similar argument as far back as 1994 because studies showed even then that screening doesn’t save lives—death rates are the same with and without it—although it may save the life of this or that individual.
But the clearest, most even-handed explanation I’ve seen for the logic behind rationing medical tests appeared in this past Sunday’s New York Times Magazine. Using simple math, John Allen Poulos showed definitively that when you test a large group of people for a relatively rare condition, you will get substantially more false positives than real ones. The wider the population tested, the more this effect is exacerbated. It’s a counterintuitive result that leads to the following question: If testing is always good, why not lower the age for routine mammograms to 30 or 20—or 12?
For good reason. Putting aside cost and risk of these tests—mammograms involve radiation, as cancer survivor Barbara Ehrenreich points out in her own response to the testing brouhaha—the answer is that lowering the screening age increases the ratio of real to false positives. And soon enough, the cumulative dangers of those false positives begin to outweigh the dangers of the real ones. They compel healthy women to undergo invasive biopsies and sometimes radical treatment for growths that may never pose real harm. Not only that, but Poulos notes that because survival is calculated from the moment of diagnosis, “ever more sensitive screening starts the clock ticking sooner. As a result, survival times can appear to be longer even if the earlier diagnosis has no real effect on survival.”
All of this stuff is true not only with mammograms but other screens, including PSA tests, which have also come under scrutiny. A PSA test measures prostate specific antigen, a protein that shows up at higher concentrations in the blood of men with prostrate cancer. The catch is that many older men have very slow-growing forms of this cancer that will never kill them. But serious consequences await those who seek biopsies and aggressive treatment—radiation, chemo, or prostate surgery. As author Shannon Brownlee noted in a recent MoJo piece, they may end up popping Viagra and wearing Depends—with little to show for it.
To actually improve health care, the government needs to consider what’s good for a population of patients, not simply what an individual patient believes is right for him. Socialism? Fair enough, but consider that all insurance, whose aim is to spread risk from the few to the many, also falls into that category. In any case, rationing is a bitter pill in a country obsessed with the individual. But if we don’t pull it together and make some tough, wise choices, it won’t just be a few unlucky patients feeling the pain.











{kind=link}