
When Owen came down with Covid-19 in April 2021, he felt lucky to get away with a mild case. After a few days of a runny nose, he returned to his regular routine, including long sessions at the gym. But three weeks later, Owen, who was 25 at the time and working as an art director in Manhattan, began to have trouble breathing. It got so bad one day that he collapsed in his kitchen. Later, at the emergency room, doctors searched for a cause but could find none, so they sent him home.
That was only the beginning of Owen’s ordeal. In the weeks that followed, he was so exhausted that he couldn’t get out of bed. He tried to work, but his thinking was fuzzy. His appetite was low, and he had trouble digesting even the smallest snacks. Doctors ran heart tests, ultrasounds, and blood counts that turned up nothing. Owen, who requested that I use only his first name to protect his privacy, visited several clinics for long-haul Covid patients. He got vaccinated. He went through cognitive behavioral therapy, a psychological approach to managing symptoms. A doctor prescribed him a low dose of an anti-addiction medication that had shown some promise in addressing the brain fog. None of it helped. Over the next few months, Owen lost nearly 80 pounds. Desperate, he scoured the internet for answers.
It didn’t take him long to find online communities of long-haul Covid support groups on Facebook, where members described his precise symptoms: the months of debilitating fatigue, the digestive issues, the breathing problems. Some had been seriously ill during their initial infections while others, like Owen, had only mild symptoms. Members who were beginning to feel better shared what had helped—from special diets to breathing exercises to elaborate and expensive treatments with supplement infusions and oxygen chambers. Owen was skeptical about most of it, but then a concerned friend told him he had read about a program that sounded more scientific than the other treatments. A former Stanford virologist named Dr. Bruce Patterson had developed a special blood test to diagnose long Covid along with what he promised was a highly effective treatment regimen. When Owen researched it online, he found entire social media groups devoted to Patterson and his diagnostic company, IncellDX. “I am HUGELY thankful to them,” gushed one fan in a Reddit group. “For the first time in this nightmare, doctors are telling me that they have things to try that they think may help me.”
Patterson’s pitch was impressive: Owen would send a few vials of blood to IncellDX’s lab, where technicians would look for evidence of elevated levels of cytokines, proteins that are thought to play an important role in the body’s immune response. The higher the patient’s level of certain cytokines, they suggested, the worse the case of long Covid. Based on those results, Patterson’s team of doctors would assign Owen a “long-hauler score” that indicated the severity of his disease. Owen would follow up with an IncellDX doctor to discuss the results and treatment. If Owen’s doctor wouldn’t prescribe the drugs—which was likely, since many of them weren’t approved to treat Covid—Patterson’s team would connect him with a special network of doctors who would.
Owen had some reservations. He knew that the process could be pricey and that his insurance probably wouldn’t cover all of it. But he was desperate. “I was pretty suicidal,” he recalls. “I was just so done with all of this.” So, after paying a few hundred dollars for the test, he sent off his vials of blood to IncellDX and waited for the results.

Two years into the pandemic, it might be tempting to throw caution to the wind and get on with life, new variants be damned. But if you’re ever tempted to do something risky—choral singing with a few dozen friends in a basement, say, or perhaps an impulsive trip to the mosh pit—you might first consider visiting one of the dozens of long-haul Covid online support groups for a quick reality check. There, hundreds of thousands of members congregate to offer encouragement and commiserate over a dizzying list of ghastly symptoms. Some haven’t been able to get out of bed for a year or more. Others find digesting food so difficult that they have to use a feeding tube to stay alive. Many have had to stop working because they can no longer think clearly. Then there are the reports of people who have been so tormented by their experiences that they have died by suicide.
The wide array of symptoms that long-Covid patients experience makes the disease especially vexing to physicians. No one knows for sure exactly what causes it, and medications that are commonly prescribed—steroids, for example, or naltrexone, a drug usually used for addiction—don’t work for everyone, even as they do for some. Why the difference? It’s not clear. Even at new long-Covid clinics at major medical centers, physicians admit that their approach involves treating individual problems—inhalers for breathing difficulty, for example, sleep aids for insomnia, or cognitive behavioral therapy for brain fog. Dr. Benjamin Abramoff, a physician who specializes in rehabilitation and directs the Post-Covid Assessment and Recovery Clinic at Penn Medicine, says the spectrum of symptoms he sees is “very, very broad.” As for treatments, so far, he says, “There’s no one size fits all.”
Patterson’s approach is different. He claims that IncellDX’s test and treatment protocols do not focus on simply relieving discomfort, but instead, the IncellDX Covid Long Haulers website says, go directly to “the underlying immunologic causes of long-haul Covid,” which Patterson believes is an overactivation of several cytokines, small proteins that play an important role in activating the immune system. The website continues, “This new research will provide critical insight into how to predict, identify and treat patients who are affected by it.”
Patterson offers a treatment protocol that he describes as being specifically tailored to a patient’s test results—often a combination of off-label medications including blood pressure medications, steroids, an HIV medication called maraviroc, and the controversial antiparasitic drug ivermectin (though in an interview, his partner, an anesthesiologist and gym owner named Dr. Ram “Yo” Yogendra, tells me the team is now moving away from ivermectin because low-dose steroids work just as well). Proof of having had Covid isn’t required to enroll in the treatment program; the team believes that many long-haul patients had been infected before tests were readily available. Recently, Patterson’s team has also begun offering their protocol to people who believe they are suffering from long-term effects of the Covid vaccines. During a 90-minute Zoom conversation I had with Patterson and Yogendra in December Patterson explained to me, “We found a very similar pathology in postvaccination long haulers as we found in Covid long haulers, even though they’ve never experienced the actual virus.”
All of this isn’t cheap. The test costs about $360, and several follow-up consults with IncellDX physicians cost $199 each. Some of the prescribing doctors in IncellDX’s network charge a fee of a few hundred dollars, and some of the medications can cost as much as a few thousand dollars a month. Because the IncellDX team says patients often must continue the drugs for eight to 12 weeks before symptoms improve, the costs can be considerable and, again, unlikely to be covered by insurance since IncellDX’s approach is considered experimental.
Yet for the nearly 14,000 long-Covid patients who have signed up for the IncellDX protocol, that’s a small price to pay for the possibility of relief. In Facebook groups, many IncellDX customers describe the experience of being “gaslit” by doctors who had dismissed their symptoms and the relief they felt from receiving test results from IncellDX that claimed to pinpoint the science underlying their suffering. They talk about Patterson and his partner Dr. “Yo” in rapturous tones. “Dr Yogendra and former head of virology at Stanford, Dr. Bruce Patterson are months ahead of the curve,” wrote one member of the long-Covid group Survivor Corps. “With doctors like Patterson we have a voice!” enthused a member of a Reddit long-Covid forum. Some patients have even declared that the team’s treatment has cured them. One long hauler from Pittsburgh told a local newspaper that before going through the IncellDX program, she had debilitating fatigue, headaches, and tremors. Since starting treatment, “The best thing is I can actually be part of my kids’ days,” she said. “Instead of lying on the sofa watching them play, I actually got to play with them and feel like I was a mom again.”

Meanwhile, Patterson has been making the rounds, publishing op-eds about his long-Covid theory in major daily newspapers across the country, including the San Francisco Chronicle, the Des Moines Register, and the Tampa Bay Times. A Bay Area ABC News affiliate claimed in a headline for a July segment on Patterson, “Lab discovers root cause of confusion, fatigue experienced by Covid ‘long haulers.’” He has also developed a long-Covid protocol that includes ivermectin with the Front Line Covid-19 Critical Care Alliance, a group that has come under fire for its endorsement of the anti-parasitic drug as a treatment for Covid.
It’s easy to see how exciting and what a relief this all might seem to a patient who has been suffering for months. And how for that patient, it would hardly matter that neither the blood test nor the drugs that Patterson’s team endorses have been approved to treat acute or long Covid, or that an anesthesiologist would be working on an infectious disease protocol and marketing it on YouTube. When I asked patients why they were so convinced that Patterson had found a cure for their misery, they told me that they had heard that it worked from other people on the internet—on Twitter, in groups on Facebook, and forums on Reddit.
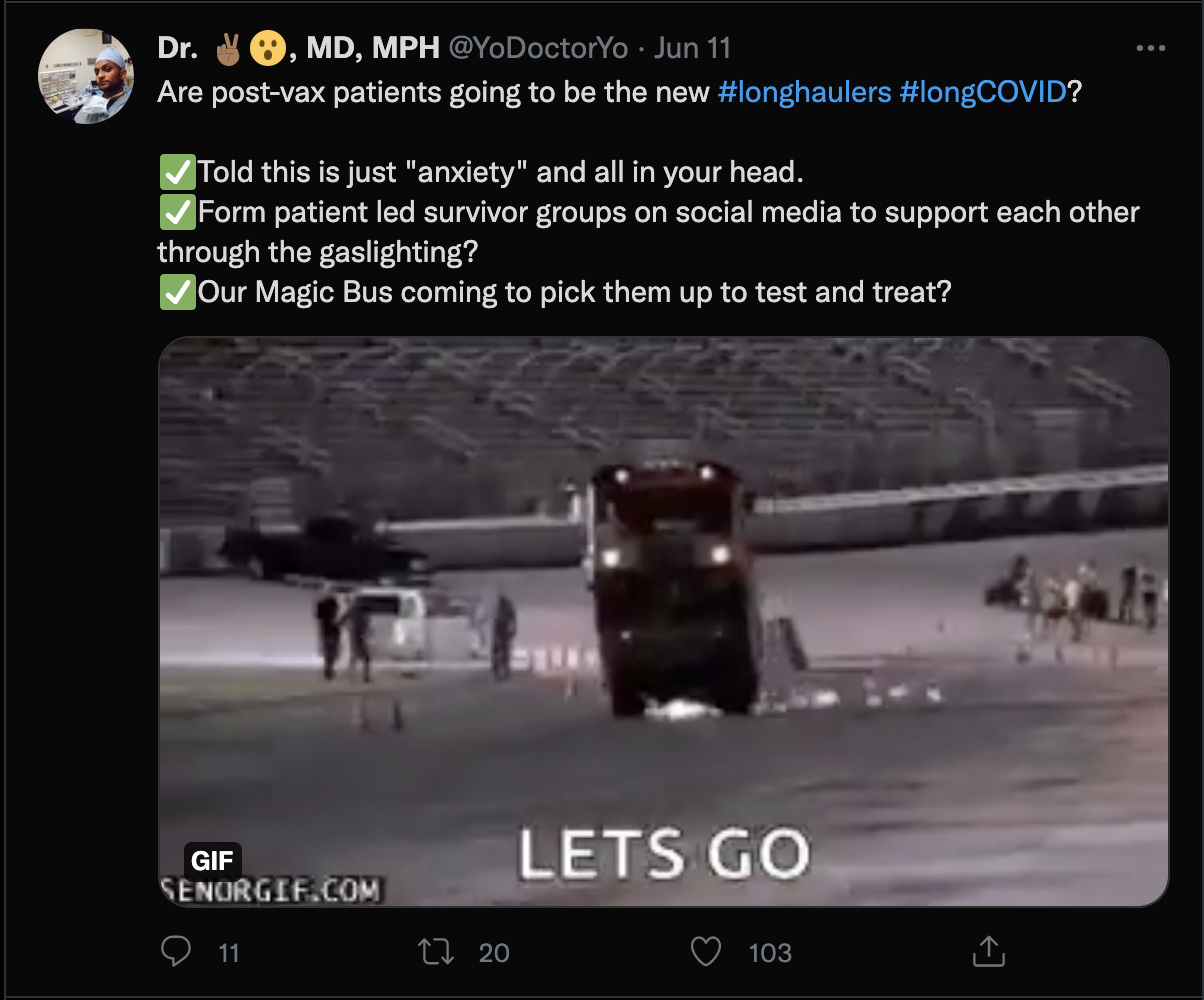
Dr. Patterson says that the protocol has worked for 85 percent of their patients. While the team has published a few small studies supporting their theory, so far, it has not conducted a randomized controlled trial, the gold standard in study design. This unconventional approach seems at times to be a point of pride. “We are the ETSY of longCovid-DIY but giving you something the establishment can’t,” Yogendra tweeted last May.
Those breathing exercises at your #longcovid clinic not really helping? Well @brucep13, @purviparikhmd and our Magic Bus welcome you to come check us out.
We are the ETSY of longCOVID- DIY but giving you something the establishment can't 🙂 pic.twitter.com/yfPQ6KA3Lw
— Dr. ✌🏾😮, MD, MPH (@YoDoctorYo) May 19, 2021
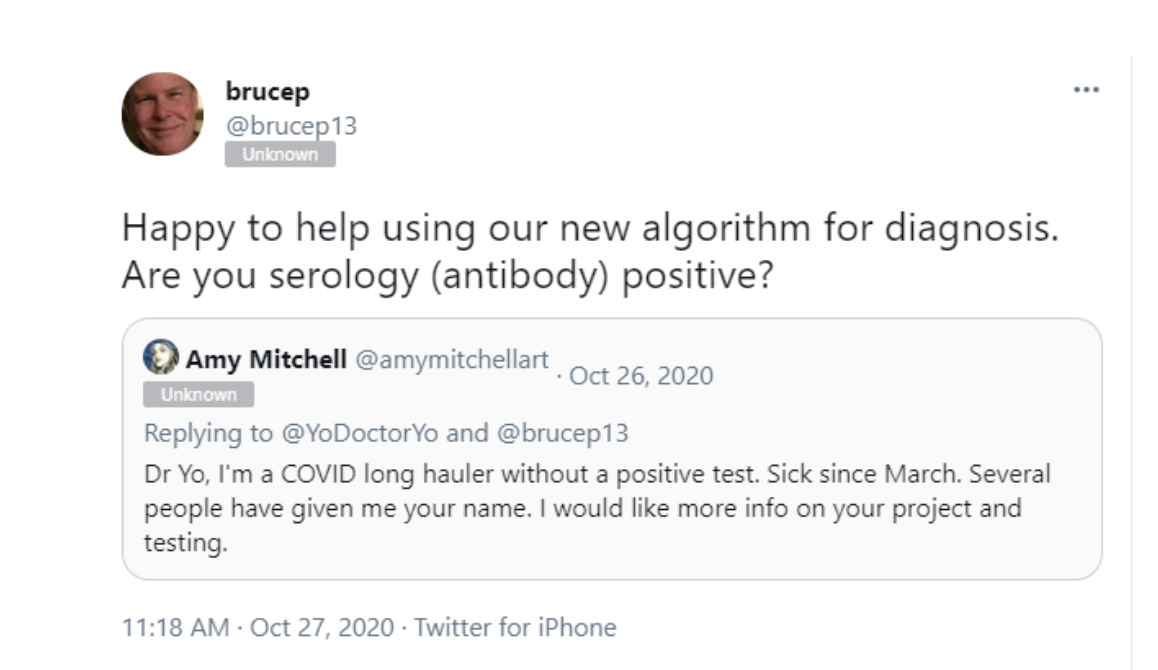
When a long-Covid patient on Twitter asked Patterson how to enroll in an IncellDX trial, Patterson responded, “It’s not a trial, we are testing and treating!” He urges patients to sign up through Covid longhaulers.com, IncellDX’s website devoted specifically to long Covid. The team also welcomes patients who have never officially been diagnosed with the disease, and whose antibody tests are negative. For Dr. Yogendra the antibody tests are irrelevant “because you might have gotten infected and never made antibodies or they just waned over time.”
This treat-first-test-later method is not the only irregular thing about IncellDX’s long-Covid work. A Mother Jones investigation uncovered unusual behavior by the team, including offering medical advice and recruiting patients on YouTube and social media, failing to disclose financial conflicts of interest, and reports of inconsistencies in lab results—all in service of a program that often costs thousands of dollars. Taken together, these practices have raised the suspicions of some scientists and patient advocates who worry IncellDX may be using unproven tests and treatments to take advantage of the desperation of 14,000 long Covid patients. As Stanford bioethicist Hank Greely put it to me, “The red flags are in full force on this one.”
Of course, such concerns aren’t unique to IncellDX. In the long slog of the pandemic, many businesspeople have seen opportunities. From repurposed drugs to questionable air filters to boutique vaccine-exemption consultants, Covid has proven to be lucrative for some entrepreneurs. Long Covid represents yet another opportunity. The potential market alone could be enormous. By some estimates, the condition will affect between 10 and 30 percent of infected patients, which might mean millions of people. And long-Covid sufferers are especially vulnerable because so little is known about their condition, says Diana Berrent, founder of the long-Covid support group Survivor Corps. She has seen many of the 180,000 members of her Facebook group spend thousands of dollars on IncellDX treatments, with, she says, no real results: “Bruce Patterson and Dr. Yo are, to me, the sketchiest guys out there.”
To these criticisms, Patterson and Yogendra counter that their approach is light years beyond what other doctors are doing. “I talk to the hospitals, and they’re still putting patients on their bellies like they did in February 2020, and shooting them full of steroids,” Patterson told me during our call. “It’s not like we’re giving toxic cancer drugs; we’re giving very rational, approved, safe drugs. And that’s the way medicine should be practiced, not the way some CMO of a hospital determines it should be.”
In August 2021, a few days after Owen had sent his blood samples to IncellDX, his results arrived in an email. The test found high levels of several cytokine markers, which the IncellDX team said indicated that Owen did indeed have long Covid and could benefit from the company’s treatment protocol. During Owen’s consultation, a staffer put him in touch with a telemedicine doctor who would prescribe a steroid, a statin, ivermectin, and the HIV medication maraviroc. The process of actually acquiring the drugs, Owen recalls, was “a nightmare.” He had to order some of the medications from China, and he paid $2,000 out of pocket for the maraviroc. But his fatigue, brain fog, and digestion problems were getting worse, so he began the treatment, crossing his fingers this investment would result in relief. To avoid getting discouraged, he began compulsively checking the internet for any new morsels of positive signs about the protocol. “I was checking Twitter for what Dr. Patterson or Dr. Yo were saying about the treatment because there’s just not that much info,” he says. The doctors, he learned, had quite a tight group of followers on social media and YouTube; it struck Owen as being a “weird, cultish environment.”
Indeed, the doctors do seem to cultivate an unusual sense of community around IncellDX. On Twitter, Yogendra often urges patients who feel abandoned by their doctors to get on IncellDX’s “Magic Bus.” In the live chat sections of their YouTube videos, the two physicians appear to revel in the attention from their audience. Some Patterson devotees called themselves the “wild bisons,” a reference to an earlier video in which Yogendra said that was Patterson’s “spirit animal.” Several members of the Bisons’ private Facebook group have told me that it is tightly controlled and that members who criticize IncellDX are censored. The group’s rules describe it as “a way to share notes, experiences, or concerns with other people who are undergoing treatment, without all the outside noise from the naysayers and lurkers in other groups.” (It also notes, “The administrators/moderators of this group do not work for Incelldx nor do they have any connections to the company besides being patients themselves.”)
Patterson’s public behavior can appear to be unorthodox for a physician. He has occasionally dabbled in the world of antivaccine media—in November, the host of a holistic health podcast called “Let’s Talk Wellness Now” asked him whether the IncellDX long-Covid treatment protocol could cure “some of the kids that have been vaccine injured with autism or brain encephalitis.” That theory—that vaccines cause autism and other brain problems—has been thoroughly debunked. Yet rather than correcting the host, Patterson simply responded, “We’re not there yet.” On Twitter, he has offered to diagnose people with long Covid using his unapproved test. He also has made unfounded claims in interviews and on social media that the drugs he endorses can treat symptoms such as brain fog, neuropathy, and tinnitus. That’s a problem, says Stanford’s Hank Greely, because IncellDX’s approach is “both unproven as a diagnostic and unproven as a treatment for this particular disease.” Still, Patterson, a highly-credentialed, genial-looking middle-aged white man, comes off as trustworthy and credible. He often appears in IncellDX videos wearing a white coat and peppers his comments with arcane explanations of the immune system, all of which confers an air of scientific gravitas.
Patterson’s serious manner stands in stark contrast to that of his partner, Dr. Ram Yogendra, who began collaborating with Patterson in 2020 after Patterson helped him treat one of his Covid patients. Yogendra often brags that he cultivates close relationships with IncellDX followers. In one April 2021 YouTube video, for example, Yogendra comments in the live chat, “i realized i have all your numbers saved on my phone. i guess i made friends all over the country because of long Covid lol.” In July 2021, he tweeted a photo of himself drawing a patient’s blood at her house. (He says he had her permission.) “Midnight calls. Texting stupid memes and gifs,” he tweeted. “I realized that the #longCovid patients are not my patients anymore…these people are my family.” Yet there’s a darker side: Yogendra flies off the handle in comments on Twitter and social media. At one point in that same April YouTube video, a commenter said that her primary care doctor questioned the results of her IncellDX test. Yogendra’s response? “[T]ell them to F off.” When I asked Yogendra about his combative tone, he told me that he feels that he has a responsibility to defend IncellDX. “Sometimes it’s just cheap shots, and I’m not going to put up with it,” he said. “I’m just not that type of person.”
Owen was not the only person to become unsettled by their unconventional approaches. Nick Guthe also got a strange feeling from the IncellDX team. Guthe’s wife, Heidi Ferrer, had been suffering from symptoms of long Covid for almost a year when she signed up for IncellDX’s protocol last spring. She was hopeful about the treatment, but Guthe told me that from the very beginning something about Yogendra’s bedside manner seemed off. His wife’s conversations with the physician often happened at odd times when Yogendra wasn’t at the office. Once, Guthe said, Dr. Yogendra called from the supermarket and offered Ferrer clinical advice as he was doing his grocery shopping.
Dr. Yogendra connected Ferrer with a doctor who, for a fee of $500, prescribed the medications from the IncellDX protocol, including ivermectin. At first, the drugs seemed to resolve some of Ferrer’s symptoms, but they came roaring back, along with even more troubling problems, including an internal buzzing sensation that left her unable to sleep. Guthe recalls the horror of watching his wife tormented by insomnia, taking Ambien every few hours to no avail. The torment of sleeplessness, the persistent internal noise, and the large doses of a sleeping aid, became, Guthe says, “a recipe for destroying your mind.”
Last May, Guthe’s worst nightmare came true. When he returned home after picking up their 13-year-old son from a friend’s house, he found his wife in the bedroom. She had hanged herself. A few days later, a grieving Guthe used Ferrer’s phone to text Yogendra. “Dr. Yo, this is Heidi’s husband, Nick, reaching out to you,” he wrote. “Heidi took her own life on May 23, pronounced legally dead on May 26. I need to share with you what happened.” In a follow-up phone call, Guthe recalls, Yogendra offered his condolences but couldn’t offer much insight. “He seemed so shocked, he didn’t offer much in response.”
Yogendra told me that he remembered the conversation with Guthe, but that he hasn’t spoken to him since. Guthe, he said, “was going to connect us with the NIH, because I think they were going to an autopsy of her brain and donate her body for research. That’s the last thing I recall.”
Bruce Patterson’s medical pedigree is impressive. During his residency in pathology at Northwestern University in the early 1990s, he made a key discovery in HIV research. In 2004, Patterson became director of clinical virology and co-director of the AIDS Research Center at Stanford. “His pioneering technologies and findings have contributed to advances in detection, prognosis, and treatment of patients infected with HIV,” a Stanford press release about his appointment boasted. In 2009, he founded IncellDX as a diagnostics company. Two years later, he left Stanford to focus full-time on the enterprise. Over the next decade, IncellDX developed tools to aid in the diagnosis of several diseases, including HIV, hepatitis, HPV, and certain cancers.
Fast forward to 2020 when, just a few months into the pandemic, Patterson developed a theory about what caused severe Covid. At the center of his hypothesis was a cytokine called CCR5, which he had studied during his work on the role of cytokines in both HIV and cancer. He theorized that when activated, CCR5 could prevent the immune system from adequately fighting off the virus. So, if there were a way to stop the overactivation of CCR5 and a few other important cytokines, Patterson reasoned, Covid symptoms should subside.
As luck would have it, just such a drug existed: leronlimab, an experimental HIV medication that worked to suppress the virus by targeting overactive CCR5 cytokines. It was manufactured by Cytodyn, a publicly traded biotechnology company based in Vancouver, Washington. It seemed like a stroke of luck that Patterson had found the very drug that would treat the Covid problem his team had identified. Except that it wasn’t luck. Because as it turns out, Patterson was already intimately acquainted with leronlimab. He was working on trials of it for HIV—as well as breast cancer—before the pandemic even started.
In 2019, Cytodyn announced that it would use a test made by IncellDX to identify HIV and breast cancer patients who might benefit from the drug. At the time, Cytodyn was running a trial for the use of leronlimab to treat a very aggressive form of breast cancer, and Patterson’s team began working furiously to recruit patients. In one 2020 YouTube video, Yogendra interviewed a British man named Adam Wright who had become convinced that leronlimab would save the life of his wife, who, at age 33, was gravely ill with stage-4 breast cancer. Wright told Yogendra that what he had learned about how leronlimab could help even the sickest patients, and the promise of it for his wife had filled him with new hope. For more than an hour, Yogendra and Wright praised the drug—despite the fact that Wright’s wife had not yet tried it. “Your story is going to be so powerful,” Yogendra told Wright. “There are going to be so many women and families and kids who are going to see a lot of hope and keep fighting.” (Sadly, Wright’s wife died shortly before she began treatment.)
After the pandemic hit in 2020, Patterson partnered with the company to work on two very small trials of leronlimab in a handful of severely ill Covid patients, and Cytodyn conducted two slightly larger trials with a few hundred patients, as well. The company reported that the drug seemed to reduce a patient’s chances of dying from the disease. Meanwhile, Patterson went on a media blitz singing the praises of leronlimab. “The fact that I’m smiling, or at least glowing a little bit,” he said in a June 2020 Ted Talk, “is the fact that this drug has saved lives.” He made these claims despite his research on leronlimab and Covid being extremely preliminary. (Indeed, a disclaimer at the beginning of the TED Talk video notes that “the drug discussed in this talk remains under clinical investigation and is an unproven therapy to date.”)
In May, the Food and Drug Administration chastised Cytodyn for making its own overblown claims about the drug and concluded: “[I]t has become clear that the data currently available do not support the clinical benefit of leronlimab for the treatment of Covid-19.” Then, in the summer of 2021, both the Securities Exchange Commission and the Department of Justice opened investigations into whether the company, which is currently valued at more than $700 million, had misled shareholders by overstating the efficacy of leronlimab in Covid patients.
At around the same time, Patterson and another colleague, Paul Rosenbaum, led an effort by a group of activist shareholders to take over Cytodyn’s board of directors. In a July 2021 letter, the group accused Cytodyn executives of having “mishandled their stewardship of Leronlimab, thereby failing to capitalize on significant opportunities to unlock substantial value for all stockholders.” The coup attempt failed. In August, the Cytodyn board rejected the takeover bid. The company then successfully sued the group for failing to disclose a major conflict of interest: Patterson, it found, had previously tried to sell IncellDX to Cytodyn. A Delaware court agreed. “The Board legitimately suspected that Patterson and others were keen on revisiting the failed attempt to combine IncellDx and CytoDyn,” the judge stated. “For Plaintiffs not to appreciate the presence of that elephant in the room reflects either reckless indifference or deliberate gamesmanship.”

Dr. Bruce Patterson
Mother Jones; Scott Strazzante/The San Francisco Chronicle/Getty
I asked Patterson about his involvement with Cytodyn. He attempted to distance himself from the activist investors, claiming that he only became involved at the request of the group. “The group that put that together and funded it wanted me as a board nominee, and I said, ‘Yeah, of course, I would be interested,’” he told me. Similarly, he said he hadn’t considered selling IncellDX to Cytodyn until the company approached him about a potential deal.
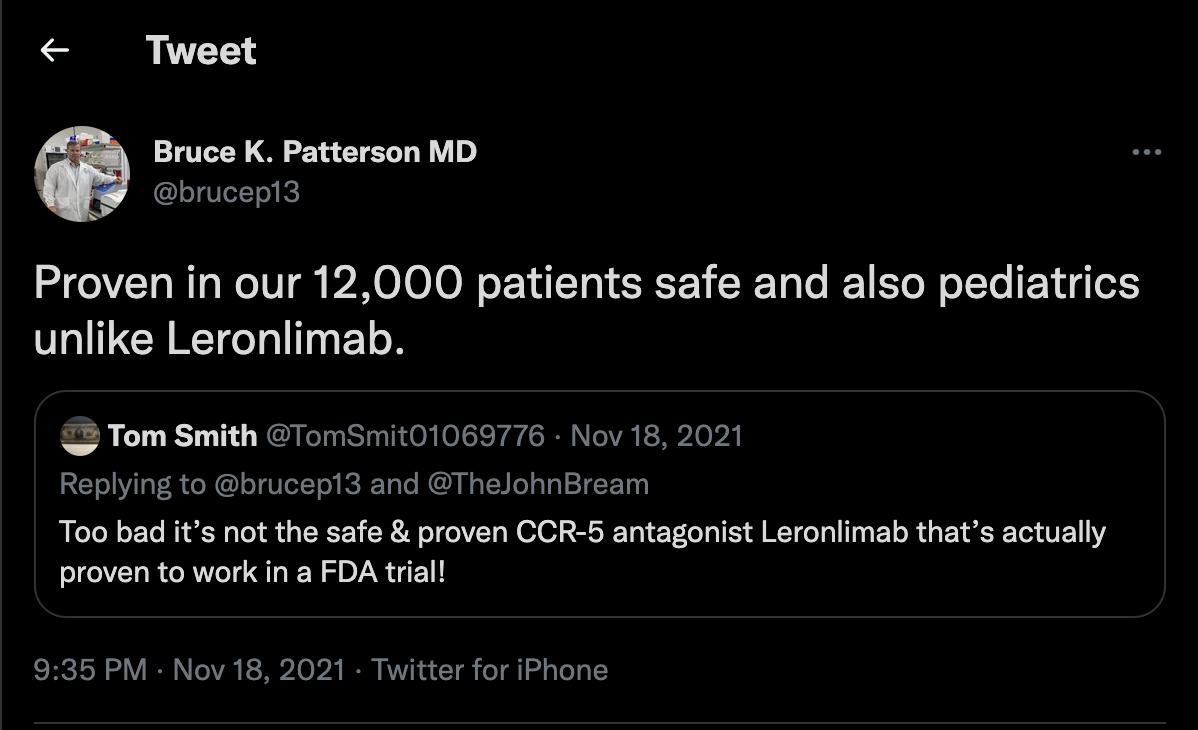
After the takeover bid went south, Patterson and Yogendra stopped mentioning leronlimab as a promising treatment for long Covid—in fact, recently Patterson has disparaged leronlimab on social media and has redoubled his praise of maraviroc, which works through a similar mechanism. Maraviroc is “[p]roven in our 12,000 patients safe and also pediatrics unlike [l]eronlimab,” he tweeted on November 18. Patterson maintains that his shift from leronlimab to maraviroc had nothing to do with his failed bid to take over Cytodyn’s board—rather, he says, it’s easier to prescribe maraviroc because it’s approved by the FDA (though not for long Covid). “My concern has always been that there are other drugs out there that are just as good [as leronlimab],” he said, adding that Cytodyn doesn’t “realize how much competition there is out there.” In November, IncellDX announced that it had obtained a patent for the use of maraviroc to treat long Covid.
Even aside from the leronlimab episode, there are other worrying signs about Patterson’s long-Covid approach. The experts with whom I spoke said the science behind it is shaky at best. As evidence for their treatment regimen, Patterson and Yogendra point to two studies they’ve published in the journal Frontiers in Immunology. I asked Maarten van Smeden, an epidemiologist and statistician at the University Medical Center Utrecht in the Netherlands, to evaluate the study that IncellDX offers as proof of concept for its proprietary blood test for long-haul Covid. The sample size of 224 patients, van Smeden noted, was small—a particularly bad sign given that the study involved machine learning, an algorithm-based statistical analysis method that typically requires a lot of data for accuracy. What’s more, van Smeden observed, the results looked “too good to be true.” Crucially, the analysis failed to provide confidence intervals, a statistical convention that indicates how sure a researcher is about a conclusion. “Even if we’d ignore the many methodological issues with this study,” wrote Van Smeden in an email, the machine-learning model “is a long way from proving there is a cytokine storm going on.”
David Gorski, a Wayne State University School of Medicine surgical oncologist who also studies the promotion of pseudoscience, added that Patterson’s “research appears to be of the preliminary hypothesis-generating variety, rather than the validating randomized clinical trial variety.” Furthermore, most of what is known about the role of cytokines in Covid has to do with acute cases, rather than the long version. Early on in the pandemic, some researchers believed a “cytokine” storm” might be responsible for the kinds of symptoms that landed people in the hospital. But even when most acute, the role that cytokines play in the disease is still murky. A literature review this year in the journal of the Society of Critical Care Medicine of anti-cytokine treatments found little evidence of their effectiveness and advised that “clinicians should uphold caution when incorporating it into treatment protocols.”
Penn Medicine’s Dr. Abramoff is skeptical of the idea that there is one simple explanation for what happens when a Covid infection triggers months and even years of suffering, let alone that a silver-bullet treatment even exists. His team is beginning to study the role that the immune system plays—“We’re still learning,” he says— but he stresses that very little is known so far about the complex interactions between the body’s own defense system and the long list of symptoms his patients experience. Abramoff says he gets many inquiries from long-Covid patients about Patterson and IncellDX. “There’s so much mystery about what causes [long Covid], and where the pathology is,” he says. It can be an enormous relief “when somebody says, ‘It’s your cytokines, these are what’s causing you to feel this way’” and offers a treatment for that specific problem. Yet many patients don’t understand how incredibly complex the immune system is, and that the cytokine explanation remains just a hypothesis.
As irregular as IncellDX’s practices may be, Stanford’s Greely told me he doubts the company is breaking the law. In part, that’s because, due to a loophole in the FDA medical device approval process, using an unapproved test to diagnose a condition is perfectly legal. (Looking at you, Theranos!) But something doesn’t have to be explicitly illegal to raise other concerning issues—specifically, Greely points to the lack of robust data supporting the test and treatments. “You’re selling a test that you’ve got no good evidence works, and then you’re using it to prescribe a drug that you’ve got no good evidence works?” He says. “To me, safety and efficacy are profoundly ethical questions.”
After two weeks on the medications that the IncellDX team recommended, Owen thought maybe he noticed a difference. “Everything, for the most part, feels like it’s at a standstill,” he wrote in a September post on Reddit. “I don’t wake up feeling worse by any means. It’s a little more predictable each day. Heart palpitations are a little less frequent, migraines are gone, but the brain fog is still there.”
But a few weeks later, not much had changed. “About a month in, I just saw absolutely no improvement,” he remembers. “There was nothing happening.” Owen couldn’t afford any more of the pricey maraviroc. He had spent thousands of dollars on treatments, with little to show for it. On the long-Covid forums, he says, “I would watch people, just like on there for four months be like, ‘I’m still on medication, and I don’t see anything, but they keep telling me to do it. So I’m gonna do it.’” In October Owen decided he was done with IncellDX. “People who are sick, they don’t really have an option.” He believes that IncellDX took advantage of him. They “just think that they’re gonna bank on us.”
Six months after his symptoms started, Owen is finally beginning to feel better. Now, when he recalls his experience with IncellDX, he remembers some early red flags he wished he had paid closer attention to. For example, a few days before he sent his blood off to IncellDX for analysis, another physician had ordered an almost identical blood test for him through the popular phlebotomy chain Labcorp. Owen was surprised when, a few days after his IncellDX test came back with elevated cytokine levels, his Labcorps results came back mostly normal.
Owen isn’t the only long Covid patient who had test result discrepancies; one member of a long Covid Slack group paid for two separate, simultaneous tests to be run through IncellDX. The results came back significantly different from each other. When that patient asked Patterson about the results, he responded that for one of the samples the lab must have used a “short draw,” when one of the vials doesn’t have enough blood to yield accurate results. But the patient said that didn’t make sense to him—he had been watching the technician draw the blood, and he likely would have noticed if one of the vials hadn’t been full. When he posted about his experience on the IncellDX Facebook group, he says, his comment was removed. “POOF! Like it didn’t exist.” When I asked Patterson about the test result discrepancies, he repeated the “short draw” explanation and said it was common for test results to differ between labs. “Part of it is patients trying to play clinical pathologist,” he says.
On November 16, Yogendra appeared in a Youtube video with great news about a new chapter in IncellDX’s story: They would soon begin enrolling patients in a long-anticipated trial of their protocol. “We can’t disclose the name of the institution,” he says, “but this is a big academic center on the West Coast.” A few days later, IncellDX announced the details of one of its trial sites. The lead physician is a Milwaukee-based oral surgeon, holistic medicine practitioner, and anti-aging doctor. Plus, IncellDX isn’t waiting for the results of the trial to embark on new projects. The team has begun to offer its treatment for several other illnesses, including chronic Lyme disease and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. It’s also expanding its services to Europe, and it’s launching a program for children with long Covid. On November 14, Patterson tweeted, “The fatigue, sleep disturbances, loss of appetite are so profound in pediatric long Covid but they respond to treatment dramatically. #incelldx.”
Meanwhile, at Abramoff’s Penn Medicine long Covid clinic, the results are far less miraculous—but he does see patients slowly responding to therapies. Medication alone often isn’t enough—the clinic also teaches patients how to cope. For those with profound fatigue, for example, “We’ve talked a lot about the four P’s—pacing, prioritizing, planning, positioning—to adjust their daily lives to compensate,” says Abramoff. His team works over the course of months to reduce their most bothersome symptoms, a process that can be frustrating because it often involves trial and error, and a little bit of whack-a-mole. Treatments often fix one symptom but make others worse. Abramoff also finds himself helping patients navigate the ever-expanding universe of people and companies peddling unproven treatments, which he finds “frustrating and sad.” One of the toughest parts of the job is telling desperate patients that there is not yet a silver bullet. “That’s what every patient wants: a universal treatment that will make their symptoms go away,” Abramoff says. Then, he pauses. “Unfortunately, we don’t have that.”











{kind=link}
{kind=link}
{kind=link}
{kind=link}