A staff member for a St. John's Mobile Clinic provided workers with free COVID-19 testing in Los Angeles this week.Ringo Chiu/ZUMA
An analysis published by the Los Angeles Times on Saturday reveals that Black and Latino Californians aged 18 to 64 are dying at higher rates than their white or Asian peers, relative to population, as the pandemic continues to highlight deep inequalities across the country.
When accounting for each group’s share of the population, black and Latino patients under the age of 65 had higher rates of fatality than even older blacks and Latinos—although people over 65 still make up the overwhelming majority of COVID-19 deaths. The trend is particularly noticeable among those age 18 to 49, the Times analysis found…
Among patients ages 18 to 49, black residents are dying nearly two and a half times as often as their share of the state’s population. By comparison, black people 65 and older are dying twice as often as their share of that age group. Latino death disparities also go down as patients get older, the analysis found.
The new reporting adds extra numbers to a powerful preliminary analysis performed by my Mother Jones colleagues Eddie Rios and Sinduja Rangarajan published mid-April, which found that Black people overall have disproportionately contracted and died from the coronavirus. In 20 of the 28 states plus DC for which a usable racial breakdown of infection data was provided, Black people make up a larger share of coronavirus infections than they do of the general population.
In 18 of the 23 states plus DC for which a usable racial breakdown of fatality data was provided, Black people likewise make up a disproportionately large share of coronavirus fatalities. In Michigan, Black people are 14 percent of the state’s population but 33 percent of its coronavirus cases and 40 percent of its deaths. In Wisconsin, Black people are six percent of the state’s population but 25 percent of its coronavirus cases and 39 percent of its deaths.
For more charts and data analysis on inequalities revealed by the coronavirus crisis, check out our in-depth reporting, here.
President Donald Trump was up early Saturday morning taking credit for sending a few ventilators to Colorado and thanking all the people in the state who allegedly sent him “thank you” notes for his benevolence. He also tagged Sen. Cory Gardner, a Republican up for a tough reelection race this year, who he has previously credited for helping with the ventilator acquisition.
But as the Denver Post has pointed out, thanks to Trump, the state actually got 400 fewer ventilators than it would have if the administration hadn’t meddled in its procurement process.
In early April, Gov. Jared Polis, a Democrat, had arranged for the state to buy 500 ventilators when the Federal Emergency Management Agency grabbed the shipment instead. Polis complained to the Post that the federal government was leaving the state high and dry. “We can’t compete against our own federal government,” Polis said. “So either work with us, or don’t do anything at all. But this middle ground where they’re buying stuff out from under us and not telling us what we’re going to get, that’s really challenging to manage our hospital surge and our safety of our health care workers in that kind of environment.”
A few days later, Trump tweeted that he was sending Colorado 100 ventilators thanks to a request from Gardner, despite the fact that Polis had been begging the feds for weeks for more medical supplies. The move was among the first of many indicating that the Trump administration was playing politics with medical supplies during the pandemic. As the Denver Post editorial board wrote:
The federal government should be procuring medicine, masks, and ventilators and distributing them to states on a set formula based on population, rate of infection and need. Instead, Trump’s messaging makes it feel as though he will watch with glee from the White House as people suffer in states being led by his enemies.
Members of Congress have demanded more information from FEMA about such order seizures and whether the distribution of masks and ventilators has been dictated by political considerations rather than need. But Trump doesn’t seem too worried about appearances. On Saturday morning, he doubled down on his earlier comments, claiming that Coloradans were so grateful they were showering him with thank you notes for the ventilator delivery:
Thank you to the people of Colorado for the warm and gracious notes and letters sent to me for all of the Ventilators we got for you. It was my great honor! @SenCoryGardner
Rules. Who are they really for? Not the president’s director of the United States National Economic Council, Larry Kudlow, whose characterizations of the pandemic have been flagrantly bullish. You’ll recall he’s the one who urged conservative activists in February, as market dread was setting in, to “think about buying the dip” to land cut-price deals, and assured investors in early March that the coronavirus was “contained” “relative to ordinary flus.”
“The virus is not going to sink the American economy,” he predicted in February. “What is or could sink the American economy is the socialism coming from our friends on the other side of the aisle.” More recently, Kudlow has been happy-talking the economy by downplaying recession fears. The US now has 26 million unemployed, and Trump just signed another aid bill, this one to the tune of $484 billion.
But Kudlow is focused on making himself look sharp for Fox News host Laura Ingraham, even if it means flouting his own administration’s social distancing advice by forcing a salon to open. Kudlow wasn’t worried. He didn’t have a temperature. He felt fine! No biggie for a round of intimate head contact with a “friend” for a “special deal”, while everyone else is growing a quarantine man bun or showing off their roots.
“I’m also going to confess, I had a hair trim yesterday. It was kind of a special deal,” he said, sitting in front of a backdrop of the nation’s capital, to an approving Ingraham hoot. “She got her hairdresser to come in and open up her barbershop and the guy gave me a pretty good trim. I don’t have much to work with, but it looks much better because I want it to look good on the Laura Ingraham show. That was the key point and here I am. I had no temperature this morning coming into the White House, I tested negative last week, I feel fine.”
Watch:
"It was kind of a special deal": White House Coronavirus Task Force member Larry Kudlow says he got a haircut to look good on Fox News. pic.twitter.com/WKx0BgoR4d
More than 50 years ago, despite a storm that was brewing in Memphis, an overflow crowd of hundreds gathered to hear a rousing speech from Martin Luther King, Jr., who encouraged the city’s striking sanitation workers not to give up their struggle for safer working conditions and better wages. “Nothing would be more tragic than to stop at this point,” he told them, in what would turn out to be his last speech.
King saw the workers’ quest as one that aligned with his national Poor People’s Campaign. When King spoke of a human rights revolution, he spoke broadly of seeking justice for people living in slums, for hungry children, and for the disenfranchised. He was fighting so that everyone could one day have a safe place to live, work, and play. He wanted “massive industries” to treat people right. “The nation is sick, trouble is in the land, confusion all around,” King said that spring night in 1968. He could have easily been speaking about the United States in 2020.
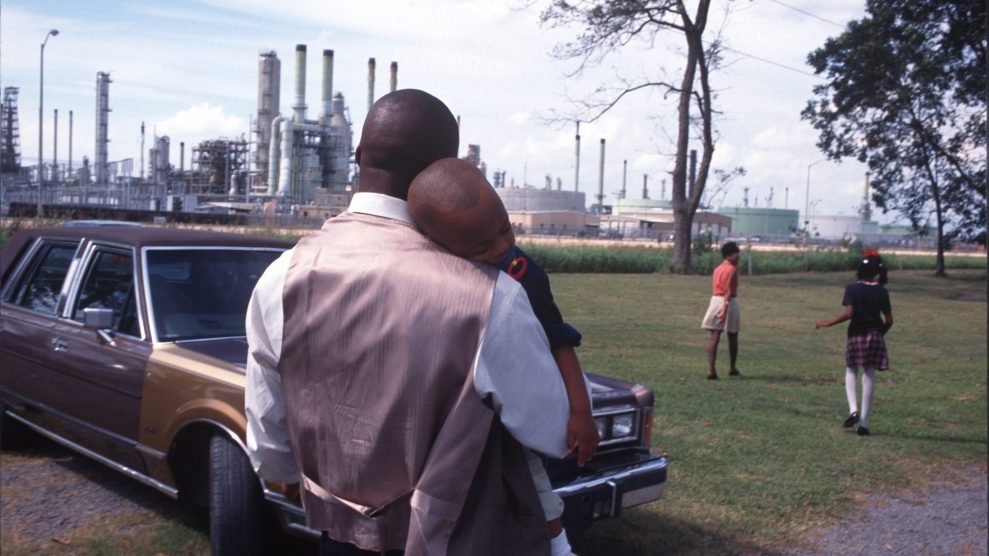
Now, as skyrocketing unemployment is predicted to increase poverty rates and widen racial disparities, these same communities find themselves in the crosshairs of COVID-19. In Chicago, African Americans represent 60 percent of the city’s COVID-19-related deaths, despite only comprising 30 percent of the city’s population. African Americans in states such as Michigan, Illinois, and Louisiana have also been disproportionately killed by COVID-19—and early data suggest the disparity could be widest in the South.
Across the country, Latinos are also feeling the brunt of the virus, with health experts particularly worried that overcrowded housing, lack of health insurance, and workplace exposure in jobs like agriculture will cause the number of cases to skyrocket. And in the Navajo Nation the numbers are grim as well, with a positive test rate that is nine times that of the rest of Arizona. Underlying issues there, including a lack of access to safe drinking water and an underfunded health care system, are putting many at risk.
The disparities send a clear message: The COVID-19 pandemic is not just a health crisis, it’s an environmental justice crisis.
Over the past month, I’ve seen in my reporting why many of these populations are so vulnerable: Farmworkers toil in unsafe conditions before returning home to overcrowded mobile homes, apartments, and houses where they cannot self-isolate. Residents who live near or work in warehouses in the nation’s logistics hubs already suffer fragile respiratory health conditions—conditions that will only worsen as pollution threatens to spike during this crisis. Environmental justice advocates who work in these communities are not surprised that the hardest hit populations are found in areas that are also overburdened by pollution, poverty, and illnesses such as obesity, diabetes, and cancer, as well as asthma and cardiovascular disease. So, when governors across the country order residents to stay home during the pandemic, these residents are not retreating to safety—they are retreating to toxicity.
Decades ago, sociologist and civil rights activist W.E.B. DuBois zeroed in on how social and environmental conditions led to health disparities betweens black and whites, and he offered solutions that addressed the physical environment. More recently, political scientist Fatemeh Shafiei, director of environmental studies at Spelman College, has studied the social conditions that determine a person’s health outcomes. She found a preponderance of evidence showing that, from cradle to grave, low-income residents and people of color are disproportionately exposed to health-threatening environments in their homes, neighborhoods, and workplaces.
Earlier this month, we heard the US Surgeon General essentially blame the drinking and smoking habits of African Americans and Latinos for contributing to the severity with which they have been hit by COVID-19—even though he noted during the same press conference that it is likely the “burden of social ills” is contributing to the disparities. He was rightly criticized for failing to acknowledge that these disparities are rooted in entrenched structural inequalities that have been in place for centuries and are the product of systemic prejudice. Long after formal segregation was struck down by the courts, for instance, targeted zoning has maintained formerly segregated neighborhoods and put them in the crosshairs of industrial pollution. It’s one of the reasons why today your zip code is still determinative of your life outcome—including your health. Geography is destiny.
COVID-19 is one more chapter in this saga, and we’re seeing that the severity of outcomes is related to a person’s environment. Public health researchers and advocates are concerned that those who live in polluted neighborhoods will fare the worst. It’s why residents are pleading for stronger air pollution regulations in San Bernardino, California, and why residents of Louisiana’s St. James Parish are battling yet another plastics plant. Not only do they not want to heighten their risk of severe coronavirus outcomes, but they also don’t want to see more friends and family diagnosed with cancer. Latinos who live in Houston’s Manchester neighborhood worry that the EPA’s relaxing of environmental enforcement will worsen the already-elevated rates of respiratory illness and asthma among residents. Navajo Nation residents want to access clean water and medical services—and not just during this crisis. As these communities fight for life during the pandemic, they’re also fighting for the right to a safe, clean environment.
King talked of the struggle to help his brethren gain their rightful place in this country, of making “America what it ought to be.” At the heart of that is the right to equal protection under the law, something that Shafiei sees as the end goal of a long history—from slavery to segregation—that has denied these vulnerable communities environmental justice by implementing policies and practices that direct pollution into their neighborhoods.
“People are being denied their equal rights,” said Shafiei. “If you look at the disproportionate number of COVID victims and the percentage of African Americans in the general population—13 percent—then that means it has really impacted their right to live.”
The right to a healthy home is considered by most Americans to be a fundamental part of the American dream, Shafiei writes in a chapter on health disparities in the first American Public Health Association book on healthy homes. But even today more than a third of housing units across the nation—37 million units—contain lead-based paint. Children of color, particularly African American children, have historically been more likely to have elevated blood lead levels, and researchers have found that racial and economic disparitiespersist today largely due to differences in environmental exposure.
We have waited far too long to address environmental injustices, and generations of Americans have paid the price. Lead exposure is just one example: Local health care agencies wait until children are exposed to lead before intervening, rather than preventing the exposure from happening in the first place. Today we face a similar challenge when it comes to addressing COVID-19 in these communities. This is why U.S. Representatives Raúl M. Grijalva, A. Donald McEachin, and Alan Lowenthal are scheduled to host an upcoming live-streamedroundtable to discuss how the fight for environmental justice can be incorporated into the government’s coronavirus response efforts.
If Americans recognize that these two battles are one in the same—and find the moral courage and political will to fix them—then perhaps environmental justice communities won’t be so hospitable to the ravages of diseases like COVID-19, said Michele Roberts, the national co-coordinator of the Environmental Justice Health Alliance for Chemical Policy Reform, which aids grassroots organizations working in communities burdened by toxic chemicals, polluting facilities, and contaminated sites.
“[Vulnerable communities] don’t have access to the protective gear, yet they have access to this virus in disparate forms and they equally have access to toxic pollution in disparate forms,” said Roberts. “Something is wrong with that.”
For Shafiei, collecting more COVID-19 data on race/ethnicity and income is key, in addition to assessing social, economic, and environmental stresses and vulnerabilities. This can help policymakers effectively direct resources to these communities. She points out that one of the obstacles to documenting the health effects of environmental hazards is the delay between exposure and the appearance of disease. With COVID-19, however, we immediately see not only how vulnerability translates into exposure, but we can also see how decades of environmental health disparities have contributed to underlying health conditions.
“COVID showed that it is the result of all these years of policies and practices that have really been detrimental to the health of minority communities and has put them at risk,” said Shafiei, a former member of the EPA’s National Environmental Justice Advisory Council from 2012 to 2018. (She also served as an environmental justice consultant for the Centers for Disease Control and Prevention.)
As we battle this disease, will we also work to find a solution to the underlying condition that plagues our country? Will we finally tear down the structural inequalities that prevent the Manchesters, the St. James Parishes, and the San Bernardinos from escaping the chokehold of industrial pollution?
In 1968, King didn’t shy away from the challenges that his generation faced. His words ring even truer today: “We have been forced to a point where we are going to have to grapple with the problems that men have been trying to grapple with through history, but the demands didn’t force them to do it. Survival demands that we grapple with them.”
As we shelter in our homes and ask ourselves what comes next, let’s remember what King told the hundreds who gathered that April night in Memphis. He reminded the crowd that they too faced a decision: whether to support the sanitation workers, even though it was not their fight. “Be concerned about your brother,” said King. “You may not be on strike, but either we go up together or we go down together.”
As families continue to lose loved ones to COVID-19 and we determine how best to help those in need, let’s not forget the other crisis that is so closely related to the pandemic’s ravages—the environmental justice crisis. As King said, nothing would be more tragic than to stop now.
In a March 22 op-ed, published just after the coronavirus had forced much of the US economy to shut down, Washington, DC, chef and emergency-food activist José Andrés proposed an elegant solution to two looming problems: Have the federal government pay idled restaurants to produce food for hungry people—”supporting millions of jobs while also feeding millions of people in desperate need.”
Andrés modeled his idea on the New Deal-era Works Progress Administration, which employed millions of out-of-work people for needed public projects, like building and maintaining roads and bridges. Since the chef published his piece, unemployment claims have spiked to staggering levels, food banks have been overwhelmed with demand, and the restaurant industry has been pushedto the edge of extinction. Yet Andres’ proposal never got traction in the US capital.
However, California’s Gov. Gavin Newsom just rolled out a miniature state-level version of a WPA for food on April 24. Called “Restaurants Deliver: Home Meals for Seniors,” the plan has two purposes, its website states:
• Help older and other adults at high risk from COVID-19 to stay home and stay healthy by delivering three nutritious meals a day, and
• Provide essential economic stimulus to local businesses and workers struggling to stay afloat during the COVID crisis.
At a press conference, Newsom added that the program will provide up to $66 daily worth of delivered food for eligible seniors, in the process supporting restaurant jobs and pumping sales tax money into the coffers of struggling local governments.
In a famous 1932 Supreme Court decision, Justice Louis Brandeis called states “laboratories of democracy,” capable of testing out ideas that can be adapted by the federal government if they succeed. The “Home Meals for Seniors” plan is worth keeping an eye on.
President Trump’s absurd suggestion that injections of disinfectants could help cure the coronavirus wasn’t, as he later suggested, a harmless stroke of sarcasm. More than 100 people in Maryland have earnestly called the state’s emergency management hotline asking about the use of household cleaners to treat COVID-19, according to Gov. Larry Hogan’s communications director.
ALERT🚨: We have received several calls regarding questions about disinfectant use and #COVID19.
This is a reminder that under no circumstances should any disinfectant product be administered into the body through injection, ingestion or any other route.
— Maryland Emergency Management Agency (MDMEMA) (@MDMEMA) April 24, 2020
Trump mused at a briefing on Thursday that disinfectant “knocks [the coronavirus] out in a minute, one minute” as Dr. Deborah Birx of Trump’s coronavirus task force hung her head in silent horror. The maker of Lysol urged consumers to not physically consume its products. And Marylanders used up valuable state resources to inquire whether they should follow the president’s advice.
The number one rule of sarcasm: It doesn’t work when you have to explain it.
On Friday, the World Health Organization announced that leaders, including German Chancellor Angela Merkel and French President Emmanuel Macron, have agreed to an unprecedented $8 billion initiative to fight the coronavirus pandemic, an effort that will include a race to develop a vaccine and ensure equal access to it.
“The world needs these tools and it needs them fast,” WHO Director-General Tedros Adhanom Ghebreyesus said at a press conference Friday. “In the past, they have not been available to all. That cannot be allowed to happen again.”
If you’re thinking that such a collaborative sentiment would be anathema to President Donald Trump—who last month attempted to buy a German company in order to gain exclusive rights to a vaccine—you’ve guessed right. “There will be no US official participation,” a US spokesman told Reuters when asked about the WHO initiative.
This, of course, tracks with every other go-it-alone, “Make America Great” decision Trump has built his presidency on, as well as his recent accusation that WHO had “severely” mismanaged its handling of the pandemic, a claim widely viewed as an attempt to divert attention from his ongoing failures in dealing with the virus. Yet amid the current pandemic—a crisis the United States leads with the highest death toll in the world—Trump’s latest refusal to participate in a global effort, what could be a vital opportunity to develop a sorely needed vaccine, is still pretty stunning. Perhaps the president is banking on his new disinfectant injections theory.
It’s come to this: The maker of Lysol and Dettol has issued a statement emphatically pushing back against President Donald Trump’s stunning suggestion that injections of disinfectants could be used to treat patients infected with COVID-19.
“We must be clear that under no circumstance should our disinfectant products be administered into the human body (through injection, ingestion or any other route),” the company, Reckitt Benckiser, said on Friday. “As with all products, our disinfectant and hygiene products should only be used as intended and in line with usage guidelines.”
The statement comes hours after Trump openly mused about what he, wrongly, thought might be the potential benefits of disinfectant injections—as well as human exposure to ultraviolet light—in treating the coronavirus. “I see the disinfectant knocks it out in a minute,” Trump said at his daily coronavirus briefing on Thursday. “Is there a way we can do something like that, by injection inside or almost a cleaning? Because you see it gets in the lungs and it does a tremendous number on the lungs.”
In one camera angle, Dr. Deborah Birx, one of the top scientists on Trump’s coronavirus task force, is seen hanging her head as she takes in the president’s remarks. The apparent shock was echoed by public health experts and lawmakers who slammed Trump for, once again, spreading dangerous misinformation amid the pandemic.
Trump has previously come under fire for his relentless promotion of the anti-malaria drug hydroxychloroquine to cure COVID-19, despite experts warning that the treatment had yet to be proven as an effective option. But in recent days, Trump has toned down that campaign, as some recent studies have suggested that hydroxychloroquine, which can have serious side effects, may not be helping patients.
Update: On May 1, the University of California, San Francisco, confirmed that all 1,845 swab tests conducted in Bolinas tested negative for COVID-19. Antibody tests—which will reveal whether anyone was previously infected—will take several weeks to analyze.
Just after 6 a.m. on Tuesday, Dr. Aenor Sawyer pulled her big red tractor into a dirt lot beside the fire station in Bolinas, California. In the lot were six white tents—”like Cirque du Soleil,” says Sawyer, an orthopedist at the University of California, San Francisco. As the sun climbed over the green hills to the east, she began preparing for the dozens of volunteers who would soon show up to pull off a feat that sounds impossible practically anywhere else in the country right now: Testing everyone in one town, whether they have symptoms or not, for COVID-19 infections and antibodies.
As the president insists widespread testing is already taking place, governors clamor for more tests, and anxious families line up in their cars overnight to wait for nasal swabs, the United States is falling woefully short of the millions of daily tests experts estimate will be needed to safely lift social distancing restrictions. But in Bolinas, an unincorporated seaside community about 30 miles north of San Francisco that’s known as an enclave of aging hippies and a retreat for wealthy weekenders, a handful of homeowners, community volunteers, and UCSF researchers managed to organize enough tests for the town’s residents, essential workers, and first responders. As of Tuesday, nearly 1,800 people had signed up for an appointment to be tested over a four-day period this week.
Researchers are hoping the project will capture rare data showing how COVID-19 may be spreading under the radar. (Bolinas had zero confirmed cases as the testing project kicked off.) The UCSF scientists will compare the results from the town to those from a similar testing effort taking place this weekend in a dense section of San Francisco’s heavily Latinx Mission District.
“Right now we’re in the middle of a pandemic that is highly infectious and has taken many, many, many lives, and we still have no understanding of how it moves and spreads through a community.” Sawyer says. “Part of that is because not everyone gets symptomatic. They don’t all end up at the hospital, and they don’t all become known cases of COVID-19. There are many people out in society that are infected, or have been infected, that are invisible.”
While testing Bolinas may have inherent research value, it would not have happened without the pull of its more affluent residents. The $350,000 project was dreamed up—and, in large part, paid for—by a handful of multimillionaires who live or own homes in town, led by venture capitalist Jyri Engeström and biotech entrepreneur Cyrus Harmon. Both were reportedly inspired by the Italian town of Vò, which brought the virus under control in March by testing every resident twice and isolating those who tested positive. They reached out to UCSF, which had recently scaled up its lab capacity with funding from the Chan Zuckerberg Initiative. “It’s this question of, well, do you just sit around and wait for the federal government to do something or do you try to take action and help?” Engestrom told the Mercury News. The first $100,000 came from Mark Pincus, founder of the mobile gaming giant Zynga.
But on the ground in Bolinas, smaller donations and “thousands of hours” of volunteerism made the project possible, says Sawyer, who started organizing logistics not long after Engestrom and Harmon reached out to UCSF. The organizers acquired protective suits from local hardware stores, gloves from restaurant suppliers, and masks from “friends who sourced them from China,” according to a blog post by Caterina Fake, the co-founder of Flickr, who is married to Engestrom. They hired phlebotomists and figured out a technique to snap lengthy nasal swabs so they would be small enough to transport. And they recruited leaders from different parts of the famously reclusive community to encourage residents to sign up online. “People do often come here to get off the grid,” Sawyer says. “So the idea of signing up for something, for some people, is just unlikely.”
In the 1970s, Bolinas’ fiercely independent residents, concerned about the ecological impact of allowing the town to grow, took control of the local public utility district and successfully froze new development for 49 years (and counting). For decades, local rebels stole the roadsigns pointing the way to town just as fast as the state’s transportation department could put them up. Now a collection of homemade signs on the edge of town warn away unwanted visitors: “Surfers stay home, save lives,” reads one; “It’s a pandemic, not a vacation,” says another. According to the Point Reyes Light‘s popular sheriff’s calls log, Bolinians have been reporting the continued presence of out-of-town surfers and beachgoers without masks.
“We call ourselves the town that fought to save itself,” Sawyer says. “That spirit has surfaced again. It’s the town that fought to test itself.”
In sight of a skatepark ramp painted “Keep Bolinas sacred,” residents arrived by car, bike, foot, and skateboard for their testing appointments. “We expected someone to come on their horse, but they haven’t yet,” Sawyer told me. As residents approached, they were greeted by volunteers who directed them around the site and handed them surgical masks in case the swabs caused them to cough or sneeze. “They told us to arrive exactly at the right time,” says Sha Sha Higby, a local performance artist, who made sure to keep her hands warm on her way to the lot so she would have good circulation for the blood test. At four different stations underneath the white tents, pairs of phlebotomists in full protective suits swabbed noses and throats for samples to be screened for infection.
The phlebotomists also used finger-prick tests to collect blood, which in the next few weeks will be analyzed for the presence of COVID-19 antibodies. Elsewhere in California, antibody studies in Los Angeles and Santa Clara County have indicated that that a far greater numbers of people have been infected with the coronavirus than previously known due to widespread testing shortages and restrictions. (The studies’ conclusions are controversial, in part due to inaccuracies in some antibody test results.)
Bolinas residents have been told they’ll learn the results of their swab tests within the week. But for people living elsewhere in Marin County, qualifying for a test can be difficult. Under the county public health department’s guidelines, doctors should recommend patients for tests only if they are showing symptoms and have had close contact with a COVID-19 patient, or traveled to a coronavirus hot spot within the last two weeks. Others can get a test if they have “moderate and persistent” respiratory illness and haven’t responded to initial therapy and their doctor can’t come up with an alternative diagnosis. Prior to the Bolinas project, Sawyer says, some first responders working in the town could not get tested despite having symptoms. The data from Bolinas might push the county and other governmental bodies to reconsider their protocols for when testing should be done, she adds.
What’s radical about the Bolinas testing project is that it includes even asymptomatic people like Higby, who has been using her time staying at home since late February to work on an elaborate lacquered costume. CDC guidelines currently prioritize testing for hospitalized patients and symptomatic health care workers, followed by people at higher risk for COVID-19 and first responders who are showing symptoms. Those without a cough, fever, or shortness of breath are considered “non-priority.” Sally Peacock, the retired owner of a stable not far from the testing site, also said she’s been feeling just fine for the last few weeks—aside from, as she puts it, the “two-in-the-morning-when-you-sneeze normal paranoia.” Her test, on Wednesday, took about 15 minutes from check-in to when she drove out of the lot.
Sawyer says the testing project reflects the culture of Bolinas—”the spirit of people contributing for the good of the whole, for the entire population, making the community better, doing what we can to fix problems here.” She notes one local woman who has been pinning free home-sewn masks to a clothesline outside the general store. On a recent night, Peacock delivered a takeout order to a resident whose car wouldn’t start. The Bolinas Community Land Trust set up an emergency fund to help residents afford rent and other necessities. The thrice-weekly Bolinas Hearsay News touts an 8 p.m. “gratitude howl” and free sourdough bread deliveries.
“We’re a little random, as a town,” Peacock says. “Things either get done, or they take forever because it takes everybody a million years to agree on anything. So if we can do it, for sure other towns can do it.”
“I’m proud of everybody. I think it’s good,” she says. “Good to be known for something besides taking our road signs down.”
On Thursday evening, after the Labor Department reported that 4.4 million Americans filed jobless claims in the past week, California announced its deadliest day since the start of the coronavirus pandemic, and New York City’s top health official estimated that a million New Yorkers have already been exposed to the virus, President Donald Trump speculated about the possibility of curing COVID-19 patients by injecting them with disinfectant or exposing the insides of their bodies to ultraviolet light.
Trump’s comments at the daily coronavirus task force briefing came after William Bryan, the Department of Homeland Security under secretary for science and technology, gave a presentation about new research into how long the virus can survive under different environmental conditions. According to Bryan, “emerging results” show that the virus degrades faster in warmer temperatures and higher humidity, and that it dies quickest when exposed to direct sunlight. However, Bryan was careful to say that it would be “irresponsible” to suggest this means summer should be a “free-for-all.” He also noted that bleach and ammonia are effective ways to kill the virus on surfaces.
Trump quickly seized on the findings to brag that he had once predicted the virus would “go away” when exposed to heat. (“I think when we get into April, in the warmer weather, that has a very negative effect on that and that type of a virus,” he said in one interview in February. “So let’s see what happens, but I think it’s going to work out fine.”) But then, of course, Trump could not resist pushing beyond what the science says, noting that he has asked DHS science officials to examine whether UV light can be used to “hit the body” or somehow used “inside the body, which you can do either through the skin or in some other way.”
“And I think you said you’re going to test that too?” he asked Bryan.
“We’ll get the right folks equipped,” Bryan responded noncommittally.
“I see the disinfectant knocks it out in a minute,” Trump continued, now entering magical thinking mode. “And is there a way we can do something like that, by injection inside, or, almost, a cleaning? Because you see it gets in the lungs and it does a tremendous number on the lungs.”
Though he was more measured than Trump, Vice President Mike Pence also tried to spin a sunny scenario, based on several factors, that “could well give us a summer respite from the coronavirus.”
(Scientists, for the record, are still unsure of how the heat of summer will affect the coronavirus. Two weeks ago, the National Academies of Sciences, Engineering and Medicine published a report saying that while some laboratory data suggests that higher temperatures and humidity levels kill the virus faster, many other factors influence its transmission between humans in the “real world.“)
At one point, Trump mused to Dr. Deborah Birx, the response coordinator for the White House Coronavirus Task Force, “I would like you to speak to the medical doctors to see if there’s any way that you can apply light and heat to cure.”
“I’m not a doctor,” he added. “I’m like a person who has a good you-know-what.”
Washington Post reporter Philip Rucker pushed back. “Respectfully, sir, you’re the president, and people tuning into the briefings, they want to get information and guidance and want to know what to do. They’re not looking for rumor.”
“Hey Phil,” Trump replied. “I’m the president and you’re fake news.”
Rep. Peter King (R-NY) laid into Senate Majority Mitch McConnell after the top Senate Republican suggested cash-strapped states struggling amid the coronavirus pandemic should consider declaring bankruptcy rather than rely on the federal government for additional emergency funding.
Speaking to conservative radio host Hugh Hewitt on Wednesday, McConnell also criticized governors, “regardless of party,” seeking “free money” during this time.
“To say that is ‘free money’ to provide funds for cops, firefighters, and healthcare workers makes McConnell the Marie Antoinette of the Senate,” King said on Twitter.
…cops, firefighters and healthcare workers makes McConnell the Marie Antoinette of the Senate.
The scathing condemnation by a House Republican comes as Democrats fight for more federal aid to be included for states in the latest coronavirus relief bill, as state budgets around the country project a staggering $500 billion loss in tax revenues from the pandemic. But McConnell this week made clear his aversion to including such measures.
“My guess is their first choice would be for the federal government to borrow money from future generations to send it down to them now so they don’t have to do that,” McConnell told Hewitt. “That’s not something I’m going to be in favor of.”
Soon after the radio appearance, his office later published a news release under the headline “Stopping Blue State Bailouts,” all but confirming the deeply partisan lens through which McConnell views general state relief amid a public health crisis.
Workers distribute food at a distribution event in FloridaWilfredo Lee/AP
As the novel coronavirus spreads through the country infecting nearly 850,000 people, killing more than 47,000, and shuttering businesses, the number of unemployed people has skyrocketed at rates not seen since the Great Depression in the 1930s. The massive spike in unemployment, with 22 million unemployed, has led to a crushing wave of people in desperate need of food; photos of families and individuals sitting in miles-long lines of cars waiting at food distribution centers in California, Michigan, and Florida have gone viral in the last several weeks.
In response to this unprecedented food crisis, senators Kamala Harris (D-Calif.), Kirsten Gillibrand (D-N.Y.), and Bernie Sanders (I-Vt.) have just introduced a bill that would expand access to the Supplemental Nutrition Assistance Program, commonly known as food stamps.
“We are in the midst of a historic economic crisis—people are hurting,” Harris said. “They are struggling to put food on the table, and existing nutrition benefits don’t get people through the end of the month.”
In 2019, 38 million people received food assistance from the federal government, which averaged $448 for a family of four. Though advocates have long called for the benefit to be expanded, it remains a crucial lifeline for individuals and families living in poverty. It also boosts the economy by allowing people to purchase groceries and creates jobs in the food and trucking sector.
The lawmakers’ Closing the Meal Gap Act would increase the benefit to individuals and families by 30 percent and allow territories like Puerto Rico, American Samoa, and Northern Mariana Islands to receive food assistance as an entitlement, instead of a block grant. Today, territories only receive grants, which are a fixed amount of money, while states receive entitlements that can be increased by the federal government based on need. Currently, able-bodied adults between the ages of 18 and 49 who have no dependents can only receive three months of assistance in a three-year time period unless they prove that they are working at least 20 hours a week. States with high unemployment rates can request waivers to exempt recipients from the three-month rule. The proposed legislation also strips away all work requirements for food assistance.
The Families First Coronavirus Act, passed by Congress and signed into law last month allows the US Department of Agriculture, which administers the program, to increase benefits during the public health emergency and temporarily suspends work requirements until one month after the crisis is over. Harris’ proposed bill seeks to make these changes permanent.
“The SNAP program provides a critical lifeline for food insecure families, but during this unprecedented crisis, the program needs more support than ever to meet the needs of every SNAP recipient,” said Gillibrand. “Not only must SNAP provide more benefits, but barriers to eligibility should also be limited in order to reach more families.”
The strict work requirements are often a burden on those needing food assistance, as I reported in December:
Despite conservative rhetoric, able-bodied adults without dependents who receive SNAP are some of the poorest Americans. According to the Center for Budget and Policy Priorities, their average income is 18 percent of the poverty line. Their average monthly SNAP benefits are approximately $165 a month. For many of them, because they are adults without children or other dependents, these are the only federal benefits they are eligible for.
Then there’s the problem of documenting seasonal and gig work. Many individuals who receive SNAP earn their incomes through a string of jobs in the gig economy, such as rideshare driving or one-day freelance projects. “It’s difficult to document that,” Hamler-Fugitt says. “Who’s supposed to certify that you’re working 20 hours?”
Last December, the Trump administration proposed a new rule that would make requesting waivers even more difficult. Advocates estimated that this would have kicked nearly 700,000 people off of the food stamp rolls beginning in April 2020. Last month, the Trump administration was still planning to implement the rule, despite COVID-19 having been declared a pandemic and businesses closing down:
At a budget request hearing at the House Committee of Appropriations on Tuesday, Rep. Barbara Lee (D-Calif.) asked USDA Administrator Sonny Perdue if he had considered delaying the rule considering the public health emergency. Perdue responded that his agency had considered delaying but ultimately decided not to. Lee noted that wages in the US remain stagnant with many people are still struggling to find work.
“If they can’t find work in an economy of 3.5 percent unemployment,” Perdue replied, “I’m not sure when they can.”
A few days after the hearing, however, a federal judge blocked the new rule, citing concern over the coronavirus. “As a global pandemic poses widespread health risks, guaranteeing that government officials at both the federal and state levels have flexibility to address the nutritional needs of residents and ensure their well-being through programs like SNAP, is essential,” Chief Judge Beryl Howell of the US District Court in Washington, DC, said. The Trump administration announced plans to appeal the decision.
In contrast, the proposed legislation aims to make SNAP more accessible. “We need to give people the resources they need to afford food during tough times,” Harris said. “No one in America should ever go hungry, especially during a public health crisis.”
Dr. Anthony Back has built a career on delivering bad news. An oncologist and palliative care doctor in Seattle, Back has been teaching providers how to have tough conversations for the last eight years as part of an organization he co-founded to prepare physicians for what can be the toughest part of their jobs.
That group, VitalTalk, has long focusedon Back’s own medical specialties, where terminal illnesses are most commonplace. But lately, his inbox has been overrun with doctors and nurses on the front lines of the coronavirus pandemic, asking a new kind of question: How should they tell their patients they can’t receive life-saving care because there isn’t enough of it?
“We are seeing this huge spike in interest, because clinicians are realizing that this big boulder is coming ahead of them and they’ve got to figure out what to do with it,” says Back. “One of the anxiety points for every clinician right now is rationing.”
Of all the numbers on the coronavirus—more than 800,000 confirmed cases and 45,000 deaths in the United States (which are roughly doubling weekly), and 100,000 to 200,000 deaths considered a victory—perhaps the scariest are the figures on supply shortages. US hospitals have approximately 170,000 ventilators, and the American Hospital Association estimates that of the 96 million Americans who will come down with the coronavirus, 960,000 will require the support of ventilators.
Physicians are already seeing the potential shortages affect their work. Some hospitals are experimenting with having two patients share one ventilator; others are instituting Do Not Resuscitate policies for COVID-19 patients. Just a few weeks ago, the head of emergency medicine at NYU Langone Health reportedly emailed his colleagues to encourage them to begin thinking about triage, advising them to “think more critically about who we intubate” and assuring them that they had the organization’s support if they choose to “withhold futile intubations.”
Yet triaging—deciding who to treat, and who not to, when resources are scarce—is not often taught in medical schools. And although hospitals commonly have policies in place for surges of patients, the coronavirus complicates things because we’re still trying to pinpoint the best way to treat it.
“We aren’t starting literally from scratch, but this is a novel disease,” says Nancy Berlinger, a research scholar at the Hastings Center, a bioethics institute. “There weren’t off-the-shelf plans ready to go in the same way that [hospitals] know how they would respond to a mass shooting, or a flood.”
In 2015, a team of doctors, medical ethicists, public health experts, and lawyers drafted ventilator allocation guidelines for New York, where, even under typical circumstances, about 85 percent of hospital ventilators are in use at any given time. The document advises hospitals to bring in “triage committees” once resource shortages emerge, whodecide which patients will get ventilators based on health data provided by physicians. First and foremost, these committees are told to consider survivability—the patients that look unlikely to live, even with medical intervention, are kept off ventilators, and the patients who seem likely to recover with the help of a ventilator get the highest priority. Each patient is supposed to be anonymized for the committee, so external factors like age, race, and celebrity don’t play a role in decision making.
The method is meant to meet public health standards of care—doing the most good for the greatest number of people—but it’s far from foolproof. “It’s not an objective criteria,” says Paul Edelson, who teaches clinical pediatrics at Columbia University and helped write New York’s guidelines. He says it’s difficult to predict survivability because there’s still so much we don’t know about the coronavirus. For example, it sometimes leads to pneumonia, which often responds well to mechanical ventilation; in other cases, patients develop acute respiratory distress syndrome, which isn’t necessarily helped by ventilators.
Outside of New York, there are differing plans on whom to prioritize if hospitals are overwhelmed. There is no national standard protocol, except for a recent directive from the Health and Human Services’ civil rights office not to categorically put elderly people and patients with disabilities at the back of the line. Complaints of such practices have been filed by disability rights groups in at least four states in recent weeks. In Alabama, for example, “mental retardation” is included in the list of exclusionary criteria in the case of a ventilator shortage.
Beyond estimating a patient’s chances of survival, medical ethicists across the country have spent years debating the most equitable approach to allocating scarce resources. Hospitals could use a randomized lottery system or allocate ventilators on a first-come, first-served basis. They could prioritize certain patients, such as health care workers (since they have increased exposure and increased need during a pandemic) or pregnant patients (since some argue they’d be saving two lives rather than just one). There’s also the issue of extubating patients: Is it ever acceptable to remove a ventilator if another patient with greater need arrives?
But each of these approaches comes with drawbacks. A lottery system may not be an efficient use of scare resources, and first-come, first-served may inadvertently privilege those with greater access to medical services, potentially leaving out rural or uninsured people. The other two options assign some lives more value than others based on non-medical factors, such as occupation and family, which could be a slippery slope to deeming a certain type of person unworthy of care.
“Some of these are observations about inequality, and some of these are about the practical conditions of an epidemic,” Berlinger says. The only hard and fast ethical rules of triage, at least to Berlinger, are that no groups should ever categorically be denied care, and individual doctors shouldn’t be forced to make these on their own.
Traditionally, doctors are expected to advocate for the best care for all of their patients, so applying that ethos to a reality in which not all of their patients can be helped is difficult. “Nobody wants to be in that position,” Edelson says. It takes a toll onfront-line medical workers’ mental health, having to relax their typical standards of care and instead consider: “What range of answers would be satisfactory? What would satisfy our need to be our need to be fair, to be equitable, to be honest?”
It’s a tough calculation.
“Doctors and nurses who are not normally involved in the care of dying patients are having to deal with a very high volume of death,” Berlinger says. She thinks front-line workers will be coping with the psychological effects of such circumstances long after the pandemic, even if they don’t have to make triage decisions. “Doctors, nurses, respiratory technicians, first responders all feel that this is something like going through combat together.”
Enter VitalTalk, which hopes to help medical workers answer those questions, especially in the wake of the coronavirus. The group has moved away from its typical eight-week online course, taught by some of its 650 faculty members, to 20-minute virtual seminars that doctors can squeeze in between shifts. The trainings are meant to improve communication for the benefit of the patient, but anecdotally, Back says clinicians have said they also help them cope with their own mental anguish.
The organization has posted free COVID-19-specific guidance online, which has been downloaded thousands of times in recent weeks by medical professionals all across the globe. The guidance offers sample language for delivering test results, explaining supply shortages, and notifying family members of a death. For explaining ventilator rationing, VitalTalk recommends this: “Across the city, every hospital is working together to try to use resources in a way that is fair for everyone. I realize that we don’t have enough. I wish we had more. Please understand that we are all working as hard as possible.”
To deliver the news of extubation: “I’m so sorry that her condition has gotten worse, even though we are doing everything. Because we are in an extraordinary time, we are following special guidelines that apply to everyone here. We cannot continue to provide critical care to patients who are not getting better. This means that we need to accept that she will die, and that we need to take her off the ventilator. I wish things were different.”
At his press conference Wednesday night, President Trump said he had just signed the executive order he tweeted about on Monday, temporarily restricting some immigrant visas—a move he framed as a needed economic response to the coronavirus pandemic that’s destroying the US economy.
“We must be mindful of the impact of foreign workers on the United States labor market, particularly in an environment of high domestic unemployment and depressed demand for labor,” the order says. “I have determined that, without intervention, the United States faces a potentially protracted economic recovery with persistently high unemployment if labor supply outpaces labor demand.”
At first glance, the order does not seem as draconian as his initial tweet implied (though, to be fair, the tweet was short on details, and it still created panic). Part of the reason may be because the initial tweet reportedly sparked a significant backlash from various business interests.
First, here’s what it does do: Effective April 23, and for at least 60 days, the United States will suspend entry to foreigners who do not have an immigrant visa already in hand.
But, here’s what it doesn’t do: Crucially, the order does not seem to apply to immigrants already in the United States who can apply to become permanent residents. It also doesn’t apply to the spouses and children of US citizens.
To get more specific, the order does NOT apply to:
Lawful permanent residents of the United States.
Anyone seeking to enter the country on an immigrant visa as a physician, nurse, or other health care professional; to perform research “intended to combat the spread of COVID-19,” or “perform work essential to combatting, recovering from, or otherwise alleviating the effects of the COVID-19 outbreak,” as determined by the Secretary of State and Secretary of Homeland Security. The exemption also applies to the person’s spouse and children under 21.
Immigrant investors under the EB-5 Immigrant Investor Program.
The children and spouses of US citizens.
Children who are “prospective adoptee” with IR-4 or IH-4 visas.
Anyone whose “entry would further important United States law enforcement objectives,” as determined by the Secretary of State and Secretary of Homeland Security.
Members of the US Armed Forces, their spouse and children.
People with Special Immigrant Visas (SI or SQ), their spouse and children.
Any person “whose entry would be in the national interest,” as determined by the US government.
While the order is supposed to be in effect for 60 days, Trump could extend it, or write and sign a new one. As my colleague Camille Squires wrote Tuesday, these restrictions add to an already long list of actions on immigration and travel that the Trump administration has taken in just the last few months.
The reason for the executive order, Trump says, is to protect American workers. Meanwhile, on April 15, his administration issued a separate order to relax requirements for temporary farmworkers under the H-2A program to “protect the nation’s food supply chain.” The move came after the farm industry’s push to continue issuing visas for foreign farmworkers because US farms, as one expert told me, would “cease to exist” without them.
In sum, while the new order is more limited than we may have expected after Monday night’s tweet, it will still prove devastating to many people. The Migration Policy Institute estimates that the executive order would block more than 50,000 green cards over the 60 day period. (It’s also worth noting that US consulates worldwide had already significantly reduced or suspended their visa appointments because of the pandemic.)
On Wednesday night, Omar Jadwat from the ACLU Immigrants’ Rights Project released the following statement: “While the order is limited in scope, President Trump’s transparent attempt to distract from his own failures with this unwarranted suspension will cause real pain for families and employers across the country. Meanwhile, he continues to fail to take obvious steps that will save lives — like releasing people from ICE facilities that cannot keep them safe from COVID-19. We all deserve better leadership than this.”
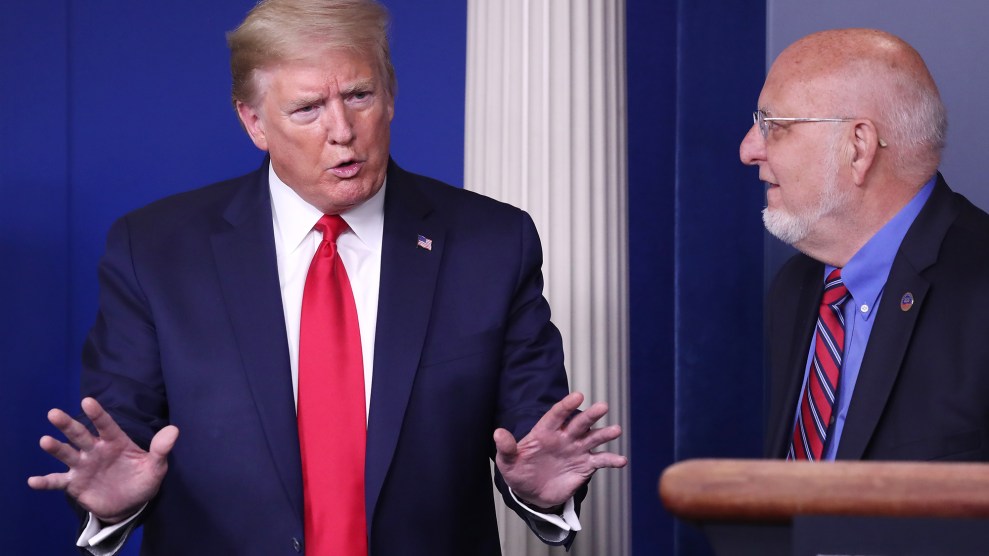
President Donald J. Trump (L) and CDC Director Robert Redfield (R) are joined by members of the Coronavirus Task Force, delivers remarks on the COVID-19 pandemic in the James S. Brady Press Briefing Room of the White House.Michael Reynolds/ZUMA
On Wednesday evening, President Donald Trump was incensed—not because of the ongoing pandemic, or, as Chris Hayes pointed out, the fact that 2,100 Americans died today, but because he felt Dr. Robert Redfield, the director of the Centers for Disease Control and Prevention, was “misquoted,” to use Trump’s words. In a Washington Post article published yesterday, Redfield warned the second wave of COVID-19 could be worse than the current wave due to it possibly coinciding with flu season.
Trump claims CDC director Redfield was "misquoted" in his comments about a second wave. He then says the quote in WaPo wasn't bad but the headline was bad. He is inviting Redfield to come up "and explain."
Sorry, to be exact, Redfield said it could be “more difficult” than the current wave, not “worse.” See the difference? Not really? Me either! But that’s the crux of the issue here: To Trump, “more difficult” does not mean anything close to “worse,” as the original Post headline paraphrased.
To be clear, Redfield did not appear to take issue with the article when it came out; he tweeted it yesterday evening, pre-Trump-tantrum.
.@CDCgov will soon issue guidance for state and local governments on how they can ease #COVID19 mitigation efforts – moving from current guidance to a phased way to support a safe reopening of America. Read more in @washingtonpost: https://t.co/bWXgznaVcF
But Trump’s plan to get Redfield to denounce the media and pour cold, cold water on the idea that there would be another severe wave of coronavirus infections pretty much backfired; Redfield explicitly admitted that he was not in fact misquoted:
6:15PM Trump on CDC Director Redfield: "He was misquoted."
6:17PM ABC's @jonkarl: "You were accurately quoted, correct?" Redfield: "I am accurately quoted in the Washington Post."
Trump just marched CDC director Redfield out to claim he was misquoted by the WaPo. But in fact, Redfield just confirmed the entire story — below — said he was quoted 100 percent accurately.https://t.co/GNnDSxWUE3
The Washington Post, for its part, does seem to have changed the offending headline from “CDC director warns second wave of coronavirus is likely to be worse” to “CDC director warns second wave of coronavirus is likely to be even more devastating,” so that’s helpful. Now aren’t we glad we took the time to clear that up?
The exchange, which left me feeling more than a little dead inside, also inspired an overwhelming feeling of gratitude to The Dixie Chicks, whose new single “Gaslighter” was the tune I chose to blast just before this whole mess started. These little gatherings sometimes truly make me question my own sanity: I slacked my editor midway through Trump’s insistence that the fake news media had screwed it up yet again, and asked, “Am I stupid, what is the problem here?” She assured me that I am not stupid, and hearing Natalie Maines belt, “gasliiiiiiighter, you liiiiiar” in my head while the “briefing” continued was oddly reassuring. I highly recommend it as a White House presser amuse-bouche.
But! I’d be lucky if I could stop there. Adding insult to injury tonight, after the failed Redfield-Was-Misquoted-Let’s-Blame-the-Media Mission, the president said he disagreed with one of his loyal followers, Georgia Gov. Brian Kemp, who this week announced he’d start to reopen the state shortly. Remember, this is just days after Trump’s tweets to “LIBERATE!!!” states from stay-at-home orders.
Pres. Trump says he told Georgia Gov. Kemp "I disagree strongly with his decision to open certain facilities,” but he has to do “what he thinks is right.”
After aggressively promoting an anti-malaria drug as a “miracle” in the fight against COVID-19—a push that flew in the face of repeated warnings from experts—President Donald Trump and Fox News personalities suddenly appear to be cooling on hydroxychloroquine just as a new study reports the drug could lead to a higher death rate.
“The fact of the matter is we don’t know,” Dr. Mehmet Oz told the hosts of Fox & Friends on Wednesday. “Thankfully these medications are prescriptions only… We are better off waiting for the randomized trials Dr. Fauci has been asking for.”
Dr. Oz, on Fox & Friends, says the VA study on hydroxychloroquine shows that "we don't know" if it works and "we are better off waiting for the randomized trials Dr. Fauci has been asking for."
Just an astonishing turnaround for a network that has been aggressively promoting it. pic.twitter.com/9EzzzNAzrQ
The segment was a head-spinning reversal for Oz, who less than a week ago encouraged Americans to participate in an at-home hydroxychloroquine clinical trial. “They mail you the pills, you start the protocol, tell them what happened… Be part of the solution,” he told Fox News viewers in a segment on April 16, the latest in Oz’s ongoing promotion of hydroxychloroquine on the conservative news network.
The attempt to strike a more cautious approach this week comes on the heels of new studies that showed hydroxychloroquine yielded no benefit in helping patients infected with the virus; one study on US veterans reported more deaths among those treated with the drug than those who received normal care.
When asked about the veterans’ study on Tuesday, Trump, perhaps the biggest hydroxychloroquine cheerleader of all, dodged.
“I don’t know of the report,” he said at his daily coronavirus briefing. “Obviously there have been some very good reports and perhaps this one’s not a good report. But we’ll be looking at it.”
The claim of ignorance appeared to track with what could be a retreat in Trump’s relentless hydroxychloroquine promotion. Politico reports that the president has significantly reduced his mentions of the drug in recent days, both in his coronavirus pressers and social media, as he shifts his focus to promoting open rebellion of Democratic governors over lockdown restrictions. Still, his repeated claims that hydroxychloroquine could be a “miracle” are unlikely to be forgotten.
HYDROXYCHLOROQUINE & AZITHROMYCIN, taken together, have a real chance to be one of the biggest game changers in the history of medicine. The FDA has moved mountains – Thank You! Hopefully they will BOTH (H works better with A, International Journal of Antimicrobial Agents)…..
On March 25, Jennifer Avalos Barrios, a 24-year-old from Guatemala with two young boys in California, made a panicked call to her sister from an immigration detention center in Jena, Louisiana. “Call my lawyer,” she said, “and tell her I’m suffocating.”
Marlene Seo, a 47-year-old who’s lived in the United States since she was 3, sent texts. “Alex,” she wrote to her daughter through an app, “they just sprayed pepper spray in here and everyone is practically dying from coughing we can’t breathe!!!” The next message was one word: “help!!!”
That morning, officials from GEO Group at Immigration and Customs Enforcement’s LaSalle detention center had assured Avalos Barrios, Seo, and their dorm mates that they were safe from the new coronavirus. Things went awry, and soon 79 women found themselves trapped in a room filled with pepper spray. They were coughing, fainting, crying out for help. It was an hour or so before they got out, Avalos Barrios later told her lawyer, Mariel Villarreal.
I’ve spoken to Avalos Barrios, five dorm mates, a woman who watched things unfold from a neighboring dorm, and many of their loved ones. Most are using their real names, a courageous decision at a time when GEO Group is retaliating against people who speak to the media.
Listen to immigration reporter Noah Lanard reconstruct the ICE pepper-spray attack in detail from interviews with several women in detention, on this episode of the Mother Jones Podcast.
Most of the interviews were done over video calls, with the women sitting in front of a backdrop reminiscent of school photo days—the realities of detention behind them obscured by a cartoonish mountain. The $0.21-per-minute calls occasionally afforded more intimacy than the phone, but they had a tendency to leave faces frozen at unflattering angles. The app we used, called GettingOut, refers to detainees by an unintentionally accurate euphemism: residents.
Even in a pandemic, getting out of the LaSalle “ICE Processing Center” isn’t easy. Nearly 1,100 of the 1,335 beds there were full earlier this month. While ICE has released some people with medical conditions that make them vulnerable to COVID-19, it continues to hold many more in tight quarters that make social distancing impossible.
The new coronavirus has brought tensions in detention centers to new extremes, but what happened on March 25 was months of neglect in the making, and ghoulish in its ironies. This is the story—in the women’s own words—of how a presentation about a virus that attacks people’s lungs culminated in guards in gas masks pulling women out of a toxic room.
Aside from the interviews with Marlene Seo, her daughter, and a woman from a neighboring dorm, what appears below is translated from Spanish. ICE and GEO Group did not respond to requests for comment.
1. Before LaSalle
Marlene Seo: I come from a blended family.
Alex, Marlene’s daughter: It’s surreal. She’s been here her whole life. Her side of the family is all Mexican. My dad is Korean. We never went to Mexico. We never visited her extended family because she was always scared of the cartel stuff.
Marlene: We have five kids and five granddaughters. This was all a shock for me—to be even sentenced to prison time for taxes. [Listen 🔈]
Jennifer Avalos Barrios: I’ve been in the US for three years. I fled Guatemala to seek asylum with my sons. They’re with my sister in California. The older one is 9. The younger one just turned 6 in February. The police arrested me after I got into an accident in Alabama. I lived in San Francisco, but I had relatives in Tennessee.
Kerlys: I’m from Colombia. I left for the capital and later got a job in the US. I was studying to be a medical assistant when I had my first daughter, who’s 7. A friend’s wife asked me to give her an implant. We ordered it from Colombia without seeing if that was allowed here. She had an allergic reaction and had to go to the hospital. The hospital called the police, then the FDA came.
I turned myself in on May 31. It was three hard months. The probation office said I wouldn’t have any issues with immigration. Then they called the next day to say that ICE had placed a detainer. ICE picked me up on August 30 and I got to LaSalle on September 5.
Adelina (a pseudonym): I’m Dominican. I’m 46 years old, and I’ve been in the US for 25 years. I’ve got five kids. I was doing tiling. I worked with a whole team—six, seven, eight, nine people for a big job. I was driving when we got stopped. Immigration status isn’t something I look into. I only care that you show up to work, but I was driving. They arrested me—took the car, my cellphone, my tools, everything. I thought I was going to get a ticket or something.
I have asthma, bad circulation, high blood pressure. But I spent a year fighting a human-trafficking charge from prison. They knew the charge would strip me of my green card. I said in court, “Innocent, innocent, innocent.” A lawyer told me they’d let me out if I pled guilty. I wasn’t getting the medicine I needed. I was having asthma attacks. What do you think I did? The judge said I was free to go. Then ICE grabbed me.
Laura (a pseudonym): I’m from Honduras, and I was living in Nashville. I’m not going to be with my son when he turns 10. When I got arrested, I said my son is asthmatic and he needs me. I said I’ve been living in this country for 15 years. The police didn’t care and called immigration. The immigration officer showed up and showed me a piece of paper. He said, “Do you know what this is? It’s your ticket back to your country.” The only thing I did wrong was coming to this country illegally. I pay my taxes.
I’ve been here for two months and will be waiting for three or four more months to have a bond hearing. [Listen in Spanish 🔈]
Mailenys Hernández Jiménez: I worked in IT in Cuba. My husband and I came to the US on May 5 and turned ourselves in together.
Mailenys’ husband: They separated us. I got sent to Colorado. She got sent to tents in the desert.
Marlene: The whole immigration process is awful, to say the least. It’s unnecessary to spend so much time in here. The depression it’s causing for people. I’m a very spiritual person. I read self-help books. I know how to stay positive. I know how to stay busy. But I just broke down today. I translate for a lot of people, so they tell me their stories. They confide in me. And it just took a toll on me today.
Yesterday, I found out that my court date was going to be changed again. I just feel like it’s so easy for them to just say “another week, another month,” when they’re not the ones in here and your families are suffering. Families are being torn apart unnecessarily. It’s sad, and it brings you down.
Kerlys: I served three months for a crime. Three months. And now I’m here for an immigration case I could handle from home with an ankle monitor. I wouldn’t be able to go anywhere because I’m on probation. But, no, we’re here in totally inhumane conditions. [Listen in Spanish 🔈]
Marlene: When you walk in, there’s tables here in the front. The beds are in the middle part, and they’re very close together. There’s seven rows. In the very back are the toilets and the showers.
Kerlys: There’s four toilets and six showers for 80 women.
Adelina: There’s only one microwave. Right now, it’s not working.
Marlene: The regular uniform is blue and orange. Blue for low level. Orange for low-medium. It’s like 90 percent blue. The other dorm has yellow and red, so they’re higher security.
Kerlys: On top of everything else that’s happening with the coronavirus, my husband left me three months ago. He said he was tired of taking care of the girls alone, and that he’d met someone else. Eight days ago, he took my daughters to Georgia. I don’t know anything about how my kids are doing, only that they’re with their dad and someone named Mary.
Adelina: I was very sick when I got here. It took two weeks to get medical attention. They thought I was playing games. They said, “Calm down, it’s nothing.” Then a doctor saw me and confirmed I have asthma.
Mailenys: Everything they give you here has flour in it. Everything. They don’t give us fruit. Today’s lunch was bread, mashed potatoes, a sweet roll, and some meat. I have a thyroid condition, so I have to eat well. There’s nothing healthy to buy from the commissary, either.
Marlene: The commissary is expensive—highway robbery for generic brand items. I saw yesterday the powdered milk is $5. It’s just a small bag. Sensodyne toothpaste is $8.10.
The cleaning supplies. I asked even before all of this. I would ask for wipes, and they would tell us we don’t have the funds. I would think that’s odd because you would think a place saturated with so many people would have common things. Then this whole COVID thing happened, and it’s like, “Okay, we really need it now.” They’re telling us we need to have it. And nope, still don’t have it.
Laura: We don’t have enough sanitary pads, soap, and cleaning supplies. They want us to keep things clean, but they don’t give us what we need.
Marlene: Hand soap. We literally had to beg for it. They’re doing a little better now. They handed us these little tubes of soap yesterday. They said they’re going to bring us one every week. When we finish one, we have to show the empty one to get a new one. But for the whole week, one little jar of soap and that’s it. It’s ridiculous.
Kerlys: We have the advantage of having TVs. We have the news on 24/7 because there’s nothing else to do.
Marlene: They don’t understand that I speak English. I kind of eavesdrop on their conversations. One of the officers said today they need to take away our TVs so that we don’t hear the news.
Kerlys: In Aliceville, I didn’t feel like I was in prison. Here, I’ve experienced what it’s really like to be a prisoner.
Marlene: I told them, we’re not criminals. We’re here just for an immigration process. You don’t have to treat us like this. They just think because you don’t speak English or whatever, they just push you along like cattle. “Do this. Do that.”
Kerlys: The guards are always outside the dorm because they’re afraid of being infected. It’s because something is happening outside that we’re not aware of.
3. La Doctora Mentirosa
Jennifer: Someone from GEO came and said that ICE and doctors were going to come and talk to us about coronavirus the next day. They said we’d have the chance to ask questions.
Marlene: They had told us not to ask silly questions. They make you feel stupid. Like, “Don’t ask about their nail polish.” I know they’re trying to joke, but this is not a funny matter.
Kerlys: The official who told us about the meeting said this was our chance to do something because things were ugly outside. She said a lot of them didn’t want to be working but that they had to. She said to only talk about the virus.
Everyone said they’re going to bring in La Doctora Mentirosa—the Lying Doctor. She’s a psychologist, but she’s known as the La Doctora Mentirosa. We don’t know her actual name. We say she’s a liar because she promises things will happen, and they never do. [Listen in Spanish 🔈]
Jennifer: It’s very difficult to talk about what happened on Wednesday, but I’ll tell you. The GEO assistant was wearing red pants, a white blouse with red stripes, and red sneakers.
Kerlys: Everything was super clean. We had our questions ready.
Mailenys: The doctor came with a plan. She was going to tell us what they wanted us to hear. But we were well informed.
Jennifer: The administrator started by introducing everyone: “She’s the doctor, they’re from ICE, he’s the captain.” She said, “I’m in charge of making sure there’s enough soap, that you have cleaning supplies, that everything is clean.”
“Perfect,” we said. “We haven’t had soap for the past few days.” She said, “Send me a request when there’s not enough soap.” Then another woman came back from court, and she said, “You’re the one who bugs me with the requests.”
Then it was the supposed doctor’s turn. She speaks Spanish very well. She said, “I’m here to talk about the coronavirus—how to avoid it, how to stop it from spreading.” She said you have to wash your hands and be more than six feet apart. You don’t have to hug. You can bump elbows.
“Any questions?” she asked. “Of course,” we said.
Laura: The question that stuck with me was one about how we could avoid being in groups of 10 or more if we have people all around us. I remember the doctor saying you have to maintain distance. The woman followed up and said, “How are we going to maintain distance if there are 80 of us?” Then the doctor dodged the question and moved on.
Kerlys: I asked what their plan for avoiding mass contagion was. She ignored me and started answering another question. I raised my hand and said, “Answer my question, please.”
The doctor said to calm down, that we shouldn’t be watching the news because it was pure paranoia. That it was a simple flu. “I have two young daughters at home,” she said. “I wouldn’t be here if it were that serious.” [Listen in Spanish 🔈]
Mailenys: She told us not to worry, that only old people get the coronavirus.
Kerlys: I read. Being in detention doesn’t mean we’re ignorant.
Jennifer: Another woman asked about people who are asymptomatic. She went to someone else. We said, “No. Answer the question.” A lot of women started saying, “You’re not a doctor, you’re a psychologist.”
Marlene: I came back from court and started hearing questions. Then so many people started interrupting. Things started getting out of control. An officer standing in the back said, “If you can’t be civil, we’re going to leave.” He called it off. Everybody got upset.
Kerlys: We hadn’t planned a demonstration or anything like that. That was just something that happened. After they left, we started to chant, “Libertad! Libertad! Libertad!” A Russian woman started yelling, “Freedom! Freedom! Freedom!”
Heather (a pseudonym for a woman in a nearby unit): I heard something about freedom. They were chanting. I’m like, what’s all this noise?
Jennifer: We started talking to them through the glass, saying that the doctor should come back. That they shouldn’t be cowards. We told a guard to open the door. We want to talk to the doctor. The guard got scared. She called a captain, who called another captain. A lot of captains showed up. They opened the door. We came up to the door. The captains pushed us. Some of the women pushed back.
Adelina: She came with a bottle of pepper spray.
Kerlys: One of the girls pushed the administrator, and a few of them took off.
Marlene: A few people got out, and at that point the administrator just started spraying everybody, then pushed the door closed.
Jennifer: It was the GEO administrator who sprayed the pepper spray. It was her, personally, who sprayed us.
Kerlys: An asthmatic woman fell to the floor after getting pepper-sprayed. She sprayed her in the face while she was on the ground.
Jennifer: She sprayed a lot people in the face, including me and a friend who’s asthmatic.
Kerlys: She did it knowing that there were people who’d had asthma attacks a few days ago from bleach they’d used in the bathroom.
Jennifer: She did it without compassion. It doesn’t matter to them that we’re humans.
Marlene: There are a lot of people with respiratory problems. We were choking from the gas. Coughing.
Kerlys: All the sudden, everyone started coughing and rubbing their eyes. It turned into chaos. Everyone coughing. The people had asthma falling on the ground and passing out.
Marlene: We were yelling for them to open the door, and they didn’t open it. Somebody threw something at the window to break it, but you can’t break tempered glass or however these windows are.
Kerlys: We were hitting the glass. Help! Help! We’re suffocating.
Adelina: It hit me in the face, too. I couldn’t see. I went with everyone else to the back. I didn’t know what to do because I’d never experienced something so terrible before. I was looking for air, and there wasn’t air. [Making a gasping sound.] Searching. Searching. It was a horror movie, but it was real. [Listen in Spanish 🔈]
Jennifer: Most of us who were up front had to go back to the bathroom.
Adelina: I saw some people jumping in the shower, so I got in the shower as well, washing from head to toe. But we still couldn’t breathe. A lot of people fainted. We were banging on the glass. Someone passed out by the door looking for air. I threw up blood.
Laura: I went up front because there was an older woman who was coughing. I wanted to help her, but when I got close, the smell of the gas hit me. I had to go back. Someone sat me down and told me to calm down, to breathe, because I couldn’t breathe.
Jennifer: I called my sister and said, “You need to call my lawyer and say I’m suffocating.” My sister said, “Calm down, you’re okay.” I said, “I’m not okay.”
Marlene: I sent a text message to my daughter: They just pepper-sprayed us. Everybody’s choking, gagging, throwing up. “Help,” is what I said.
Alex: My heart just dropped. She wanted me to call the cops, so I called the cops for their area. They didn’t do anything. They just said I needed to call the ICE processing center. They gave me attitude and said if I had a problem I should file a complaint online. [Listen 🔈]
Marlene: They came back in wearing gas masks. They were only pulling out the people who were really sick. “Bring her over here!” They were standing by the door. They didn’t want to go and get them. Then they closed the door again.
Heather: It was seeping through the door. When the door opened, the spray came inside. Everybody started coughing and coughing.
Jennifer: They said the rest of us would remain inside. We said no because we were all choking.
Marlene: They shut the door for an hour.
4. “The Animals Get Airtime, and the Immigrants Don’t”
Jennifer: They sent us to the yard, along with some of the other dorms near ours because the spray got into all the rooms.
Marlene: They took us outside, single file. They had us sit down by the fence.
Jennifer: Five captains, two guards, and two from ICE.
Marlene: They counted us all and started treating people who were really bad. They were pouring water on gauze so anybody could wipe their face. They were pointing people out who were involved. I think they told this one girl they were going to question her. She said no, no, no.
Mailenys: She’s tiny. Very skinny.
Jennifer: They told her she was the leader. We said, “There’s not a leader here. We’re all united. We all need answers to the questions we asked. We need the doctor to come back.” The doctor didn’t come back. Three men from GEO threw the woman to the ground. They put their knees on my friend’s back. If they’d pulled harder, they would have broken her arm. It was bent back.
Marlene: It took like a few people to hold her down. The men had their knees on her back. They took her, and all I remember is the way that they were holding her in handcuffs, with her hands way above her head. They were just dragging her.
Jennifer: The captains picked her up by the arms like she was an animal. [Listen 🔈]
Laura: I cried seeing how they treated her. She’s a human being, a woman. I felt very sad for her and scared they might do the same thing to me.
Marlene: Then they brought us all back inside. They came in, turned on the vents, and opened a window. The air was blowing in, and [they] just kind of let it run for the rest of the day to get the smell out of here. And that was it.
Laura: Six or seven people got here last night. They said they hadn’t been tested. Nothing. We don’t know if they might be infected. Now they’re with us.
Marlene: Everybody’s problem is that they keep bringing people in. It’s like, do you not get it? We’re already scared as it is. Louisiana is a high point of extreme contamination.
Laura: How can they not have some heart and release us so we can fight our cases from outside? We’re mothers. With everything that’s happening right now with the coronavirus, why don’t they let us out?
Kerlys: If the virus gets in here, it’s going to be chaos. We’re all going to get sick.
Marlene: We hear what’s on the TV. We hear all the rules that are being applied out there, but not in here. We’re being forgotten. They had this whole episode about animals and shelters. What about immigrants? The animals get airtime, and the immigrants don’t. [Listen 🔈]
Kerlys: They treat us like animals, but there are officials who are good, who are excellent, who are sweet. I work in the laundry. Monday to Friday, I make $3 a day washing the men’s clothes.
There’s a woman in charge whose last name is Garden. In Spanish, garden is jardín. I call her Señora Jardín. She tells me things are horrible out there. I don’t understand why they don’t let you out—to go home and be with your families—because we don’t know when this will end.
5. Getting Out
Not long after these conversations, ICE reported that a detainee at the detention center had tested positive for COVID-19. On Tuesday evening, it reported two more cases.
Late last week, Jennifer was granted a bond of $10,000. Her relatives, left without work by the coronavirus, could afford to pay only about half of it. Villarreal, her attorney, frantically secured the rest from nonprofit bond funds. They were in a race against time. The plan was to get Jennifer out before her final hearing on Tuesday.
On Saturday, Jennifer’s sister, brother-in-law, and two kids set off from California’s Bay Area at 6 a.m. When I reached her sister on Monday, she told me they’d gotten on the road at 3 a.m. after dropping the boys off at their grandmother’s place in Rome, Georgia. They were on track to complete in 60 hours a nearly 3,000-mile drive that takes 44 hours if done nonstop. At 10:17 p.m. on Monday, with Jennifer released and back in cellphone range, I got a call.
The voice on the other end—the “hola” that stretched out into two long syllables of joy—had new life to it. I asked how she was doing. Jennifer’s response was succinct: “I’m happy to be out of that hell.”
President Donald Trump speaks in the James Brady Press Briefing Room of the White House, Tuesday, April 21, 2020,Alex Brandon/ AP Photo
Last night, President Trump tweeted that he planned to sign an executive order to “temporarily suspend immigration” into the United States in response to the coronavirus pandemic.
In light of the attack from the Invisible Enemy, as well as the need to protect the jobs of our GREAT American Citizens, I will be signing an Executive Order to temporarily suspend immigration into the United States!
At his press conference today, he seemed to dial back the tweet: The executive order will only halt permanent residency applications, or green cards, for the next 60 days. (Trump did not specify which type of green card applications would be affected.) He will not suspend visas for temporary farmworkers, critical to the nation’s food supply and company’s bottom lines, he said.
But even if the restrictions are more limited than advocates had feared, let’s not forget what Trump has already done on this front. In recent months, his administration has all but shut down immigration into the country already. Since January 31, the United States has:
Closed land borders with Canada and Mexico and restricted border crossings to essential travel.
Blocked undocumented migrants and asylum seekers from entering the country.
Suspended routine visa services at US consulates and embassies worldwide.
Closed US Citizenship and Immigration Services, which processes visas, thus halting a number of immigration procedures in the US, including asylum interviews and naturalization ceremonies.
Postponed all immigration hearings under the Migrant Protection Protocols program (otherwise known as “Remain in Mexico”), leaving thousands of asylum seekers waiting at the southern border while their cases remain in limbo.
Continued flying deported migrants back to their home countries, sparking at least one coronavirus outbreak in Guatemala.
Trump paints the immigration crackdown as an effort to help the common laborer. The order to restrict new green cards is an effort to “protect the American worker,” Trump said during the presser. “It would be wrong and unjust for Americans laid off by the virus to be replaced with new immigrant labor flown in from abroad.”
In a country where immigrants make up 17 percent of the labor force, of course, immigrants are common American workers. But that’s not really what he means when he says “American worker,” is it?
Trump is expected to sign the executive order tomorrow.
A dozen nurses, standing six feet apart outside the White House on Tuesday, called on the Trump administration and Congress to allocate proper personal protective equipment for health care workers who desperately need them.
The nurses, represented by the National Nurses United, demanded that Trump invoke the Defense Production Act to require the private sector to manufacture PPE, which is in such low supply across the country that many health care workers have had to reuse equipment or simply improvise their own.
“Nurses are raising our voices across the country, and we demand to be heard,” one nurse said. “President Trump, Congress, and all other government officials: We demand that you immediately give PPE to nurses, doctors, and health care workers on the front lines of this pandemic. If you don’t protect us, we can’t protect our patients.”
Another nurse read the names of 50 nurses who have died from COVID-19.
The coronavirus has killed at least 50 nurses in the US. Now nurses are demanding the Trump administration and Congress allocate adequate personal protective equipment for health care workers who desperately need them: "If you don't protect us, we can't protect our patients." pic.twitter.com/GqhvtJvZEj
President Trump, Republican governors, and right-wing protesters are antsy to lift social distancing guidelines and return to business as usual. But a new proposal for reopening the economy while protecting the public from the coronavirus shows just how far we have to go before we can safely return to something resembling normalcy. The “Roadmap to Pandemic Resilience,” issued yesterday by Harvard University’s Edmond J. Safra Center for Ethics, calls for massively scaling up testing, contact tracing, isolation, and quarantine before implementing a phased economic recovery. That’s a tall order, especially when you consider how little testing the United States is currently doing.
While we wait for a COVID-19 vaccine, the report’s authors write, we must rapidly ramp up testing if we want to reopen the economy sooner than later:
We need to deliver 5 million tests per day by early June to deliver a safe social reopening. This number will need to increase over time (ideally by late July) to 20 million a day to fully remobilize the economy. We acknowledge that even this number may not be high enough to protect public health.
But the United States is a very, very long way off from testing 20 million people a day—much less by late July. We are currently doing about 150,000 tests a day, and at the rate we’re currently going, we’ll be doing just 530,000 tests a day by the middle of summer.
To get a better sense of just how far we have to go, here’s that same data plotted next to the Harvard report’s recommendations.
The report’s authors acknowledge that their proposal is exceedingly ambitious. They say it would require the federal government to set up a Pandemic Testing Board to kickstart the production and administration of more tests, including setting up 30 “megalabs” to analyze results. Such a program, which they liken to the rapid expansion of arms production during World War II, would cost $15 billion per month. Without it, they estimate that the economy could remain shuttered for as long as 18 months, at a cost of trillions of dollars.
Beyond its logistical and financial demands, such a program would require the Trump administration to concede that it has not done nearly enough to expand coronavirus testing. On Meet the Press last weekend, Vice President Mike Pence claimed that “we have a sufficient amount of testing to meet the requirements of a phase one reopening” and said we could “be doing hundreds of thousands of more tests per day in a very short period”—if states stepped up to oversee more testing. The president—who had promised six weeks ago that “anybody that needs a test, gets a test”—insisted at yesterday’s White House briefing that “we’re in very good shape on testing and we’re getting better all the time.”
And we respect that! But maybe you’re of a mind to support our work directly instead? We have until December 31 to raise the last $400,000 we need to keep our nonprofit newsroom running at full strength into 2026. Will you make a gift today?
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
Billionaires own the media,
but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.
Billionaires own the media,
but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.