Journalistic custom requires us to pretend that this is not a call to insurrection but rather an unfortunate case of “rank partisanship.” But Trump on Friday evening left little doubt what he was getting at in the tweets. They were directed at three Democratic governors in three states that are battlegrounds only in the metaphorical sense, for now. He said that certain lockdown measures were “too tough.” But when pressed on his “LIBERATE” tweets he cited gun control legislation recently signed by Gov. Ralph Northam. As we’ve reported, those controls were long expected. In fact, they helped turn the state legislature blue in the NRA’s backyard.
“They want to take their guns away,” Trump explained of his tweets. “That’s the Second Amendment. That’s Virginia. You have a governor—I guess he should be under siege. He seems not to be. If he were a Republican, he would be under siege. But he seems to have escaped something that is really bad…So when you talk about ‘liberate’ or ‘liberation,’ you can certainly look at Virginia.”
Trump on his "LIBERATE" tweets basically calling for civil unrest in a number of states with Democratic governors: "I think some things are too tough." pic.twitter.com/v7ff67Fiac
It appears Trump was moved to write his “LIBERATE” tweets by a Fox News segment about protests outside the office of Minnesota’s governor. These were part of a string of recent demonstrations against state social-distancing measures. On Wednesday, fashy protesters with at least one Confederate flag blocked the streets outside Michigan’s state Capitol, chanting “Lock her up!” in reference to Gov. Gretchen Whitmer.
Asked about these protests, the president dismissed concerns that they might be creating risks of disease transmission. “These are people expressing their views,” Trump said, as if viruses observed the First Amendment. “They seem to be very responsible people to me. But they’ve been treated a little bit rough.”
Here, then, were the marching orders from Friday’s press briefing: be nice to the people defying a rule to help us all not die from the plague; lay siege to the governor of Virginia.
Ricky Jones, operations manager at Magic Valley Quality Milk Transport, walks out the door as 4,100 gallons of milk pour down the drain Wednesday, April 8, 2020, at the Azevedo Family Dairy in Buhl. With restaurants across the country closed, milk processors have lost a significant chunk of their market, leaving dairy farmers with no one to take their milk. Pat Sutphin/AP
When social-distancing measures put the US restaurant industry on ice last month, the farmers who supply it saw a massive market suddenly vanish—and many had to let perfectly good food go to ruin. (In non-pandemic times, Americans spend more than half of their food dollars of meals prepared outside the home.) Meanwhile, the unprecedented spike in unemployment made millions of people unsure of where their next meal would come from, causing huge lines at food pantries nationwide.
On Friday, US Department of Agriculture secretary Sonny Perdue announced a program to address both issues at once—one I suggested a week ago (although I doubt the former governor of Georgia is a Mother Jones reader). Attending President Donald Trump’s daily coronavirus press conference, Perdue announced that the USDA would buy $3 billion worth of “fresh produce, dairy, and meat products,” to be “distributed to Americans in need for food-bank networks, as well as other community and faith-based organizations.”
Perdue didn’t mention in it the press conference, but in statement emailed to journalists Friday, the USDA announced the purchases would be delivered to food banks in “pre-approved boxes of fresh produce, dairy, and meat products.” The release offered no details about the boxes. It’s unclear whether the administration plans use this new program to test out the idea of replacing cash food aid with pre-packed “harvest boxes”—a concept widely reviled by anti-hunger advocates as inefficient and disrespectful of recipients.
On top of the food purchases, Perdue added, the USDA will spend $16 billion “in direct payments to farmers, ranchers and producers who experienced unprecedented losses during this pandemic,” Perdue added. He offered no details on how the department would decide which farmers qualify for the payments. During Trump’s trade wars in 2018 and 2019, the administration handed a total of $8.6 billion in direct payments, mainly to soybean growers who had seen exports to China plunge because of high tariffs imposed by China. An analysis by Environmental Working Group found that 10 percent of recipients—many of them wealthy owners of large farms—received more than half of the allotted funds.
Earlier this week, hundreds of demonstrators blocked the streets of Lansing, Michigan, and defied an executive order from Democratic Gov. Gretchen Whitmer to shelter in place to combat the spread of the coronavirus.
The whole charade was facilitated by the Michigan Conservative Coalition, a conservative political group that doubles as a front for Michigan Trump Republicans, and promoted by the Michigan Freedom Fund, a conservative group with ties to Education Secretary Betsy DeVos, a Michigan billionaire philanthropist power broker before she joined the Trump administration. The Detroit Free Pressreported that the fund was listed as one of the protest’s hosts on Facebook. The organization also promoted the event on Facebook.
The rift between Whitmer and the groups over the protest emerged on Monday when Whitmer criticized the Michigan Freedom Fund, saying the nonprofit “is funded in large part by the DeVos family,” and adding that “it’s really inappropriate for a sitting member of the United States president’s Cabinet to be waging political attacks on any governor, but obviously, on me here at home.” Greg McNeilly, chairman and founder of Michigan Freedom Fund and a longtime adviser to the DeVos family, tweeted that Whitmer was “misinformed and disconnected with reality.”
In a Wednesday op-ed for the Detroit News, McNeilly followed Trump’s lead in calling for easing restrictions on social distancing and demanded that Whitmer unveil her plan for re-opening the state. Michigan, mind you, is wrestling with more than 30,000 confirmed cases and 2,227 deaths from the coronavirus, with Detroit at the epicenter.
As Mother Jonesreported in 2014, McNeilly served as a longtime political adviser to Dick and Betsy DeVos and a former executive director of the Michigan Republican Party. He managed a campaign against a ballot measure that would’ve enshrined collective bargaining rights in Michigan’s constitution. Here’s how that played out (the DeVos mentioned below is Dick Devos, scion of the Amway fortune and husband of Betsy):
That summer, a group of GOP lawmakers and business leaders—McNeilly won’t say who—asked DeVos and Weiser (who served as finance chairman for the Republican National Committee in 2012) to lead the charge to defeat Proposition 2. They gladly took on the job—DeVos called Prop. 2 “a head-shot at Michigan’s recovery”—but they had bigger things in mind: With McNeilly, who managed the anti-Prop. 2 campaign, DeVos and Weiser sketched out a strategy to defeat the measure, then use the political momentum to pass right-to-work immediately afterward. They also strategized about every other possible obstacle: defending the law from a possible legal challenge, beating a constitutional amendment to repeal it, and protecting Republican lawmakers from recall elections.
They began the anti-Prop. 2 effort in September. Polls showed that 60 percent of voters supported the measure, but DeVos and Weiser tapped their national donor networks, hauling in millions from Las Vegas gambling tycoon Sheldon Adelson, Texas investor Harold Simmons, and a slew of Michigan business groups. Ten DeVos family members pitched in with a combined $2 million. The DeVos-backed campaign ran hundreds of ads in the two months before the vote, claiming the measure would give unions far too much power, cost the state more than $1.6 billion, and imperil student safety by making it impossible to fire negligent teachers.
By Election Day, the two sides had spent a total of $47 million, making it the most expensive ballot measure in Michigan history. Voters defeated Prop. 2 by a 15-point margin. DeVos and Weiser wasted no time moving to the next phase of their plan.
In a series of odd tweets, President Donald Trump called for the liberation of states controlled by Democratic governors in what my colleague Inae Oh described as the “latest signal that social distancing has fully warped into a culture war, one that depicts Democrats as oppressors willing to sabotage the economy and perhaps, in turn, the president’s reelection chances.”
TikTok thrives at the cross-section of human ingenuity and shamelessness.
Built upon musical.ly, TikTok lets users edit videos with the precision of iMovie and post with the perceived stakes of Instagram. It has spawned vlogs, memes, Drake songs, and a teen community living in an LA mansion. Its extensive search and explore features—like letting users search by the sound used in a video—mean endless scrollable content.
A multi-week quarantine has created the perfect sleepover like conditions for the app’s best content. From one-off jokes to trends made popular by the youths, here are few worth a laugh:
Dr. Fauci has become TikTok’s newest pandemic crush:
Users are using a sound from the recent season of RuPaul’s Drag Race to show off their indoor couture. (Click on the sound to see hundreds of more outfits from other users.)
Highlighting zillennial humor at its best, user @fillinthe_____s expresses the irrelevance of the stock market to an everyday young person in a compact 15 seconds.
Lizzo, the content queen she is, encouraged people to make some pretty badass remixes of her songs and showcased a few of the more banging ones. Her TikTok presence is enough to keep your mind off the rest of the world (for a bit).
User @zliang has been documenting his father’s gardening escapades—which are probably one of the most wholesome things you’ll see during quarantine. (Watch him sling a hose like a lasso or strike a pose with a watering can.)
Nothing may be more relatable than the need to just let it all out. People have been sharing in their pent up aggression with a summer camp-like chant:
Tabitha Brown has become TikTok’s vegan mom. Brown interjects vocal affirmation and encouragement into her delicious vegan recipes making her profile a beacon of hope in these trying times.
Users have long used lip-syncing as a way to poke at Trump. But with Trump’s briefings only becoming more manic, his audio has become a way to fantasize about life pre-COVID-19.
As the death toll from the coronavirus pandemic continues to rise, thousands across the country—many of whom were seen wearing MAGA hats and chanting “lock her up” in reference to Michigan Democratic Gov. Gretchen Whitmer—took to the streets on Wednesday to protest stay-at-home orders that states have put in place to curb the spread of infections.
This looks like a still from a horror movie. It's not. It's yesterday outside the Ohio Statehouse. Incredible shot by @joshuabickelpic.twitter.com/wZFye9YTCX
The scenes were a kind of depressing manifestation of President Donald Trump’s own frustrations with the public health crisis and the social distancing measures—largely endorsed by his own administration—that he blames for tanking the economy. The hellish timeline continued on Friday with the president blurting out in quick succession:
The trio of tweets, which target states controlled by Democratic governors, is the latest signal that social distancing has fully warped into a culture war, one that depicts Democrats as oppressors willing to sabotage the economy and perhaps, in turn, the president’s reelection chances. The increasingly partisan dynamic comes as Trump’s poll numbers continue to slide amid his botched handling of the crisis.
Perhaps not surprisingly, Trump’s outburst seems to be linked to a segment he saw on Fox News.
Minutes after a Fox News segment on a protest against social distancing measures outside the Minnesota governor's office, by conservative "Liberate Minnesota" group, Trump tweets "LIBERATE MINNESOTA!"
J. Khadijah Abdurahman, a single parent living on Roosevelt Island in New York City, works full-time as an independent researcher focusing on race and surveillance technologies. In 2011, Abdurahman started fostering her four nieces and nephews. Eventually she adopted all of them, and they joined her biological son, who was born in 2008. Her three sons and two daughters range in age from 5 to 13. Each attends a different school, and they all have disabilities. Abdurahman and her kids share their two-bedroom apartment with Abdurahman’s mother, who also works full-time as a nurse practitioner at Memorial Sloan Kettering Cancer Center and helps take care of the kids. Pre-coronavirus, getting all of the kids to school in the morning and coordinating their child care after school was a carefully orchestrated operation. Now, Abdurahman and her mother are focused on helping them coexist in tight quarters while they attend virtual schools.
On Friday, March 13, the day after the World Health Organization declared the coronavirus a pandemic, and a week before New York City Mayor Bill de Blasio made the decision to close the city’s public schools, Abdurahman kept her kids at home. “It felt like public schools were going against World Health’s guidance,” she said. Now, they’ve all been learning online for about a month, with materials she describes as “asynchronous,” meaning that they are receiving and completing their assignments without the real-time supervision of an instructor. Abdurahman has been spending 20 hours a week managing her children’s virtual education in addition to her full-time work, which has also gone remote. Since the start of quarantine she’s launched a new “We Be Imagining” podcast,an outgrowth of her work on an eponymous project at Columbia University, about the intersection of race, tech, surveillance, and COVID-19. One of the episodes focused on “NYPD’s surveillance apparatus, the spread of COVID in Rikers Island and what it means to police the pandemic.” She retreated to a space beneath her daughter’s loft bed in order to record it.
I caught up with her to find out what it’s been like juggling five virtual educations from the epicenter of the coronavirus. Our conversation has been edited for clarity.
On her oldest daughter:
Her 13-year-old daughter attends Democracy Prep New York Charter Schools in Harlem. Her distance learning platforms are Zoom and Google Classroom.
The week that the city closed schools, they rolled out their virtual platform. Mainly it seems to be successful. The only bump in the road was when the gym teacher requested they take videos of themselves working out, and I was like, absolutely not. She might be failing gym, but I’m not having my 13-year-old daughter sending videos of her jumping around to a male gym teacher.
Most of her virtual school is asynchronous. She has Zoom classroom advisory meetings twice a week, but the rest is just a set of assignments and the workload in general is pretty low. She probably spends 10 hours a week on schoolwork. I’m actually thrilled with her school because I just think that it’s not realistic to think they’re going to be learning tons and tons of information. Plus, she’s been panic baking— making cupcakes, cheesecake, butter cookies, hamantaschen. I’m just like, yeah, I can work with this.
Part of the whole model of charter schools is that they’re hyper-obsessed with college. They started college tours in the seventh grade. But that said, Democracy Prep has the highest suspension rate in the city. I only put her there because it was almost 100 percent Black, and I felt like they had better expectations for her than the predominantly white public school that she went to.
On her oldest son:
He’s 11-years-old and in sixth grade at the NYC Lab School—a public secondary school. His distance learning platforms were first Zoom and Google Classroom; then Zoom was banned by the NYC Department of Education, so the school switched to Microsoft Teams.
His school is pushing me towards a nervous breakdown. He’s high-functioning on the autism spectrum and is in a program which is a partnership between the DOE and NYU to create these specialized, integrated co-teaching classrooms. He goes to this really highly competitive, top-rated public school, but he’s within this specialized program for kids on the autism spectrum. My main concern is that he’s really difficult. He’s vehemently opposed to school in general. He hates virtual school, and he’s transparent with them. He told them he’s grieving the loss of all of his independence.
Now he has a full 9 a.m. to 2 p.m. schedule of virtual school. He gets a checklist of seriously weighted assignments to complete every single day: reading responses, science quizzes, math worksheets…The majority of it is asynchronous. The only synchronous portions are office hours and lectures from 10 a.m. to 1:30 p.m., with a half-hour lunch break. He does not want to do it at all. I try to monitor him, but besides not having time, in his defense, it’s like watching paint dry. I mean, it’s extremely unidirectional, no interaction. They’re just lecturing at him. Especially for kids with disabilities, he doesn’t have those organizational skills to review the work and come prepared with questions. And so they’ll reach out to me, because he’s facing his Google Meets calls to the wall, and walking away. He’s often logging off the calls. They email, text, and call me constantly because of either inappropriate comments that he’s making on Google Classroom, or emails that he sent school-wide saying, “It’s COVID time, I’m not doing this.”
In their defense, I think they only had 36 hours or something like that to put together a virtual learning program. But it was really evident that they just threw this together. And they have no sense of humor. For example, they have these questions to verify his attendance. They asked him, “Are you here today?” And he wrote “No.” So they contacted me, saying, “He’s not here, is everything okay?” And I’m like, he’s joking around. How could he select no if he wasn’t there? Guys, come on.
My concern was that since he goes to such a hyper-competitive school, and there’s such a high rate of compliance among those people, he will be identified as an outlier. Since all these people are paranoid about abuse right now, I did not want him to be labeled as truant, and have the Administration for Children Servicesor anything else involved. I’ve been keeping documentation. Maybe there’s one other Black kid. He might be the only one.
On her middle son:
Her middle son, who is 8 years old, should be in the second grade but, as his mother says, he’s “not in any kind of school right now.”
He had autoimmune encephalitis, or “brain-on-fire” and was attending a partial hospitalization program. So when I decided to keep him home on that Friday [before the city closed schools], they automatically discharged him. He had a notice to be placed in a specialized classroom in our local public school. I reached out to start enrolling him there, but it’s been radio silence, even from the Board of Ed. He’s been doing really well at home. I mean, it’s kind of crazy that he’s doing well in the midst of a pandemic.
Previously he was going to a prep school, so I reached out to them, and they’ve been much more responsive. He might go back there, but they just went on spring break, because unlike public schools they’re still honoring spring break. So I’m waiting to hear back from them.
On her youngest son:
He attends first grade, with other 6-year-olds, at Gillen Brewer School on the Upper East Side. Google Meet is his distance-learning platform.
He goes to a private elementary school that’s all special education. He has high anxiety and now all of these environmental accommodations that really helped him self-regulate are totally gone. We’ve lost all these relationships and structure. So he spends a lot of time running around like Chicken Little. And to keep him calm is like its own job on top of everything else.
His school started doing classroom meetings that were synchronous over Google Meet. It happens daily at nine o’clock. Seeing his friends and seeing his teachers every morning, keeping a relational connection, is helpful. I don’t necessarily think that it enhances his learning, but it’s comforting, and it adds a level of structure. The classroom meeting is 30 minutes, and then he has about 30 minutes of activities. But they’re easy. Like, when you’re eating snack, the kids have a conversation about what happened today.
The thing that I appreciate about his school is that they were—look, our entire school is designed to have these highly trained professionals working with your kids at a “10 to one to three” ratio. This is not going to be like that. There’s no way that we can translate the school to virtual. I think everybody with special needs cases are already super overwhelmed. Now they’ve created an at-home learning program that they upload to Google Classroom. They have therapists so that you can sign up for therapist calls, but honestly, I wrote them today saying, “I cannot implement this.”
On her youngest daughter:
Her 5-year-old daughter attends pre-K at Lenox Hill Early Childcare Center, where the kids use Zoom.
She was attending a Head Start program. They feed the kids three times a day, and they predominantly serve a Hispanic and Central American population. Head Start is based on your income, so you have to be within a certain percentage of the federal poverty line. This is definitely a population of people they were worried could lose childcare, food. And a lot of people don’t have internet access or access to computers. I think pre-K in general hasn’t had virtual school. This week the teachers started doing check-ins, and they’re trying to do a classwide Zoom call once a week. But basically, it’s been nothing. They just send us emails with links for online games and stuff like that.
On her own workload:
I tried early on in the game to implement all these learning activities. But honestly, it’s just really challenging. Given the economically precarious climate, it feels like I just have to prioritize working because I don’t want to lose income when I have five other people besides myself to provide for. I don’t know how anyone could possibly micromanage all this virtual learning while working full-time, cooking 21 meals a day, making homemade masks and cleaning, and dealing with people in my life who are dying from COVID. It’s just totally impossible.
This is a crisis. It is a pandemic, and especially for single parents with multiple children, and then on top of that, their disabilities. It’s non-viable for us to implement some rigorous curriculum, on top of working and just the entire stress of the situation. I would say the thing that’s most horrifying to me is that, anecdotally, I hear that people are still having Children’s Services call on them. And I worry that if you cannot adhere to these unrealistic expectations that you could be subject to further surveillance, and potentially even incarceration. It’s just like a third layer of stress. But, in the end it’s like low-expectation theater.
On social distancing:
We take a walk at least once a day, but it does get a little dry because the parks are all closed and we live on Roosevelt Island, which is kind of visually unstimulating. Sometimes we walk all the way south. And sometimes we walk all the way north. But it’s like the same thing over and over again. And then we have to carefully plan it because it’s an island. There’s not a lot of square footage for the 14,000 people. So social distancing is difficult.
Plus we’re trying to make homemade masks. The kids, who don’t like to wear masks, have to wear masks. I think the first week was okay, but we’re definitely getting to a point where everybody is high-anxiety. A lot more tantrums and kind of going nutty.
On how she’s managed to keep her energy up:
A lot of coffee. A lot of Red Bull.
On how she’s stayed sane:
Making the podcast, reading books by Black folks, loving on my kids.
Albert Dowdell wears a protective mask on a bus during the COVID-19 outbreak in Detroit.Paul Sancya/AP
The coronavirus deals out death and despair unequally across America. Scientifically speaking, the virus can infect anyone. But as epidemiologist Camara Jones recently toldMother Jones, “the disease discriminates in how profoundly those people are affected.”
In early April, Mother Jones began requesting racial and ethnic breakdowns of COVID-19 infections and deaths from health departments in all 50 states and the District of Columbia. Of those, 21 states released no racial or ethnic breakdowns of those infected. Twenty-six states failed to release breakdowns of fatalities by race, and among the states that did, the information was inconsistently formatted. Some broke out data only by race, others only by ethnicity, and some by both. Some offered data for Latinx and Asian communities; others classified them as “Other.” Most states had little if any information about how Latinx, Asian, and Native American populations have been affected.
But a clear picture did emerge. Preliminary data analysis by Mother Jones finds that Black people overall have disproportionately contracted and died from the coronavirus. In 20 of the 28 states plus DC for which a usable racial breakdown of infection data was provided, Black people make up a larger share of coronavirus infections than they do of the general population.
In 18 of the 23 states plus DC for which a usable racial breakdown of fatality data was provided, Black people likewise make up a disproportionately large share of coronavirus fatalities. In Michigan, Black people are 14 percent of the state’s population but 33 percent of its coronavirus cases and 40 percent of its deaths. In Wisconsin, Black people are six percent of the state’s population but 25 percent of its coronavirus cases and 39 percent of its deaths.
Similar data for Latinx populations is hard to come by. What we do have shows that Latinx people are dying at much higher rates in New York City relative to their share of the population but not in any of the places that provided relevant breakdowns.
Civil rights groups, medical professionals, and lawmakers have pressured the Centers for Disease Control and Prevention to release data on who is infected and who dies from the coronavirus by race and ethnicity. The CDC has since released racial data on 10 states.
There is no one cause of the racial disparities, says Thomas LaVeist, dean of the Tulane School of Public Health & Tropical Medicine. The list of possible culprits is long. Black Americans are more likely to work jobs that are considered essential—they’re grocers, fast-food workers, transit and postal workers. As a result, they risk greater exposure to the disease. Black people in the North tend to live in dense, historically segregated cities—Milwaukee, St. Louis, Detroit, Chicago—in which disease can spread quickly. Black people in the South, Louisianans excepted, live in states that did not expand Medicaid, leaving many of them uninsured. (A Mother Jones analysis found that six of the country’s 10 most vulnerable states, according to something called the “COVID-19 Community Vulnerability Index,” are located in the South. In Mississippi, where 90 percent of counties are particularly vulnerable, Black people make up 38 percent of the state’s population and a startling 66 percent of COVID-19 fatalities.) Owing to factors like the siting of toxic dumps and new highways, Black people suffer disproportionately from underlying health conditions such as asthma and heart disease that elevate the risk of death in coronavirus patients.
“We can’t forget how racially segregated this country is by design.” LaVeist says. “This is an outward manifestation of structural racism where African Americans are at an increased risk.”
Citing the disparities in disease rates and outcomes between Black and white Americans, Clyde Yancy, chief of cardiology at Northwestern University’s Feinberg School of Medicine, calls this a “moment of ethical reckoning” in an editorial in the Journal of the American Medical Association. He points out that infection rates were three times higher in counties with mostly Black people than in predominantly white counties.
What’s more, predominantly Black counties saw a sixfold higher death rate than mostly white counties. “A 6-fold increase in the rate of death for African Americans due to a now ubiquitous virus should be deemed unconscionable,” Yancy writes.
“The scourge of COVID-19 will end, but health care disparities will persist.”
An occasional series about stuff that’s getting us through a pandemic. More here.
The one thing that eluded me was a thermometer.
As anxiety about the coronavirus grew and store shelves started to thin out, I tried to stay one step ahead of the curve. No hand sanitizer to be found in the Bay Area? No worries, my parents sent me some from my hometown. No more Lysol wipes? I’ve been stocked for months. Face masks? Got it. While remaining careful not to unnecessarily deprive others of critical supplies, I meticulously acquired flu medicine, ibuprofen, rubber gloves, backup prescriptions—everything I thought I’d need to wait out the pandemic at home.
But with fever being one of the most common symptoms of COVID-19, I, like everyone else, wanted to be able to take my temperature regularly. Local pharmacies and big box stores were long cleared out. I scoured reputable sites, less reputable sites, and my own mental Rolodex in search of a thermometer. (This included reaching out to an ex-boyfriend who works in medical supplies looking for an inside connect; that was a mistake.)
It is a thermometer designed to take an infant’s temperatures with minimal disruption. The brand seemed legit, and it was in stock at an affordable price. Add to cart.
The sense of vindication I got at having finally completed my coronavirus arsenal far outweighed any embarrassment I felt at being a 20-something childless woman purchasing a baby item. Who needs pride when you’re prepared?
Even in normal times, I respond to situations mundane and stressful alike with a clear plan of action (and also at least three backup plans of action). I bring sunscreen to the beach. I bring a jacket to the park. I have the Google Maps route pre-loaded on my phone. My prepping hasn’t yet elevated to the level of doomsday, but, sure, I’ve bookmarked sites with instructions on how to build a bug out bag.
This intense need to plan ahead for every possible situation is, of course, a thin façade for the fact that in reality, I’m baby. Despite any outward projections of confidence, I hardly know what I’m doing most of the time. Being prepared is a part of my general fake-it-till-you-make-it approach to adulthood. All I really want is to be enveloped in a warm hug and told by a trusted authority that everything will be ok. And right now, who wouldn’t want that?
The coronavirus crisis has put our powerlessness into stark relief. There is so much we can’t control. It’s reasonable to focus our energy on the little that we can. In this new reality, dyeing your hair is okay, becoming a chicken farmer is okay, and—in the face of an enemy as frightening and unknowable as a global pandemic—buying a pacifier thermometer is okay. It’s even a win.
By the way, the pacifier works. As soon as the package got to my house, I opened, sanitized, and popped it in my mouth. A minute later, it chimed with a reading: a perfectly normal 98.6.
In this 2017 photo, chef Thomas Keller puts the finishing touch to a caviar dish in the new kitchen at the French Laundry restaurant in Yountville, Calif. The celebrated chef had just opened a state-of-the art new kitchen at his famed French Laundry after spending $10 million on an extensive renovation. Eric Risberg/AP Photo
The coronavirus lockdown has put the US restaurant industry on life support. Insurance policies for business interruptions aren’t paying out. The Paycheck Protection Program (PPP), the part of the recent stimulus act available to help restaurants stay alive and keep their workers paid, has already run out of money—even though less than 10 percent of the available $350 billion went to food-service establishments. Millions of restaurant workers have been laid off.
But if you fear your favorite neighborhood eatery will be gone when the COVID-19 nightmare ends, the Trump administration has news. On April 14, it rolled out the “Great American Economic Revival Industry Groups,” charged with charting “the path forward toward a future of unparalleled American prosperity” after the coronavirus threat ebbs.
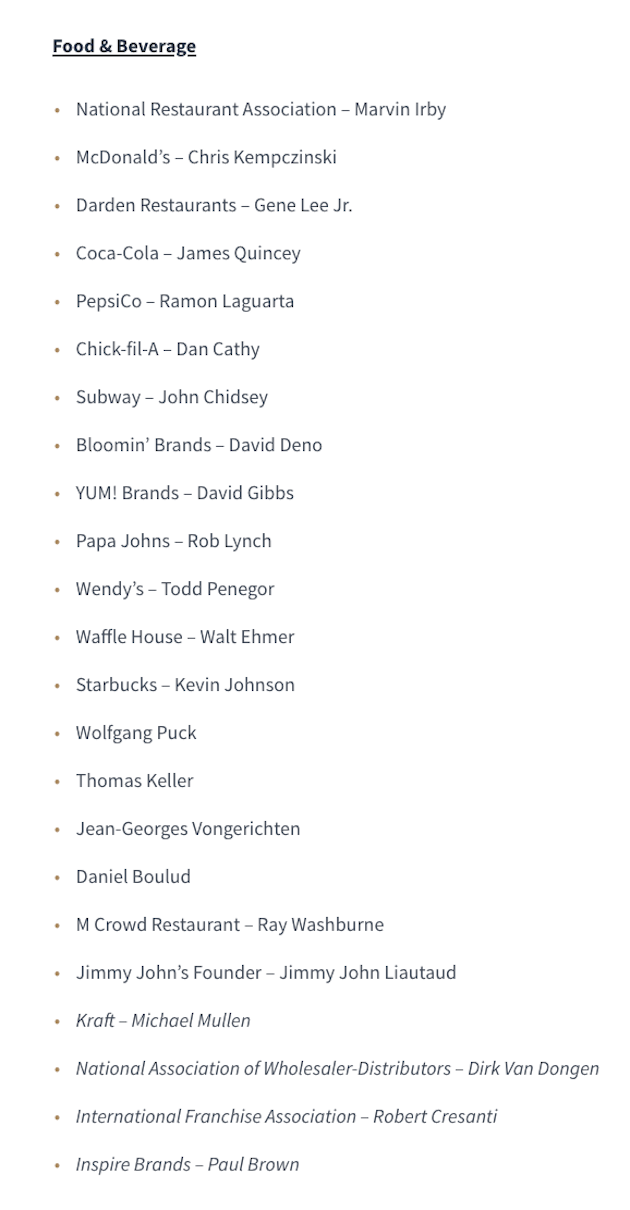
And here’s who Trump chose to represent the nation’s diverse food and beverage industries:
In short, male execs from a bunch of corporate brands—including sugary drinks giants Coke and Pepsi—plus four white chef-owners from ultra-expensive, globe-spanning restaurant groups: Wolfgang Puck, Daniel Boulud, Jean-Georges Vongerichten, and Thomas Keller. Small establishments, like the ones that made Queens, New York, into a culinary jewel, have no representative on the committee.
Vongerichten has an active business relationship with Trump. His restaurants Jean-Georges and Nougatine are located within the Trump Hotel in Manhattan, and also supply room-service meals to guests. Vongerichten’s Trump Hotel operations recently suffered a tragedy. Jesus Roman Melendez, a Mexican immigrant who worked as a cook at Nougatine for 20 years, died of COVID-19 in early April. Grubstreet’s Chris Crowley eulogized Melendez as the “backbone of one of New York City’s most acclaimed restaurants.”
For his part, Keller, proprietor of expense-account temples in Northern California, New York City, Las Vegas, and Miami is proud to be involved with Trump’s new group.
Honored @realdonaldtrump asked me & @danielboulud@wolfgangpuck@jeangeorges to join @whitehouse Great American Economic Revival Industry Group. Proud to work together towards a strategy where the safety of Americans is top of mind in conjunction towards economic revitalization.
It’s not clear whether Puck, Boulud, and Vongerichten share Keller’s enthusiasm. On April 16, the New York Timesreported that some business leaders “had no idea” they were included on Trump’s Great American Economic Revival Industry Groups team, “until they heard that their names had been read in the Rose Garden on Tuesday night.” And “others who were willing to connect with the White House could not participate in hastily organized conference calls on Wednesday because of scheduling conflicts and technical difficulties,” the Times reported. I have reached out to Puck, Boulud, Vongerichten, and Keller to for comment, and will update this post if I hear back.
In the meantime, like so much else about the administration’s response to the COVID-19 crisis, the revival effort for restaurants looks like a typical Trump Administration move: It highlights institutions that cater to the wealthy, and corporations that have made billions by selling cheap, unhealthy food to the rest of us.
Ding dong, it is eight o’clock in the east and today, like so many days in the recent past, that means that the leader of the free world strutted into the White House press briefing room and delivered an update about the pandemic gripping our nation. Why? To soothe his people, allay the fears rumbling in their bellies and the anxieties echoing in their bones, and to—dammit all—just get out the truth.
What is that truth? Something about how things aren’t his fault and that states are a board game?
Trump on state-by-state reopening: "I call it: a beautiful puzzle. You have 50 pieces. All very different…But when it's all done…a very beautiful picture."
Trump repeated what’s been the Trump line for this last little bit of time that the country will reopen soon because it wasn’t built to be closed and everyone is clamoring to hangout in groups again.
Trump: "America wants to be open and Americans want to be open."
He convened a council of plutocrats to advise on said opening, but the ultimate reality is that he doesn’t have the authority to lift quarantine restrictions.
This is, again, Trump suggesting he has made a decision to let states do something they don't need his permission to do. (He could have tried in various ways to make governors' lives difficult, but he never had the power to lift their restrictions.) https://t.co/uTrKPTbTIa
Earlier in the day, the White House released some guidelines about when it would be good to reopen. These are suggested notes to governors. Apparently they weren’t well received.
This isn't a plan. It's barely a powerpoint. — No provision to ramp up testing — No standard on levels of disease before opening ("down" is a direction, not a level) — No protections for workers OR customers pic.twitter.com/bE3GCYeECw
Trump went on tonight to tout his incredible progress—unbelievable progress, the best progress in the history of the world—that allows these states, all very different, all very individual puzzle pieces, to reopen on their own schedule. And he said that it’s such impressive progress that he thinks 29 states will reopen soon—though he didn’t name them—but his position cannot be reconciled with one stubborn reality: The country needs more testing to open back up. But! But! But! Testing has actually declined in the last week! As Politico explained on Tuesday:
The number of coronavirus tests analyzed each day by commercial labs in the U.S. plummeted by more than 30 percent over the past week, even though new infections are still surging in many states and officials are desperately trying to ramp up testing so the country can reopen.
Testing is the key. Testing is the silver bullet. We have be told for weeks that it is being scaled up; indeed, if you woke someone in the night and asked them what “incredible progress” means they would very likely tell you that it means more testing.
So how do you square that circle? How do you make that work?
I don’t know the answer. And I didn’t see one in this press conference.
What I did see is this: someone trying to lay the foundation to blame everyone else. To blame governors, China, the wind, the willows, and the lilies that did not labor or spin:
Drivers for Lyft and Uber in both San Francisco and Sacramento protested from their cars Wednesday morning, circling government buildings to demand the state award them expedited unemployment insurance and back wages amid the coronavirus pandemic.
But the point is broader: Gig workers are agitating the state to recognize them as employees.
On January 1, Assembly Bill 5, a law that was supposed to make it harder for gig companies to classify workers as independent contractors, went into effect. But tech companies haven’t complied and the state of California hasn’t done much to enforce it. Major delivery companies have poured $110 million into a ballot measure to overturn the law come November. And they’re still moving forward with the initiative—even as the coronavirus has exacerbated concerns of precarious safety and pay from workers.
“I’m doing everything I can do to enforce AB 5,” said Michael Frazier, a driver in Los Angeles who called into a Zoom press conference from his car after the protest, a white mask hanging over his chin.
Drivers say they are owed back pay for lower than minimum wage payment, expenses, and overtime. Over 2,500 drivers have already submitted claims totaling more than $630 million in back wages, according to Rideshare Drivers United (RDU), who organized the protest this morning. And RDU is helping drivers submit their unemployment assistance with the state—a benefit only employees had until the recent federal pandemic unemployment assistance—hoping that will force California to recognize drivers are not independent contractors.
But Uber and Lyft have refused to report driver’s income to the state, blocking unemployment claims. And drivers say that when they’ve filed as employees with the California Employment Development Department, the state told them they qualified for $0 in assistance.
“It’s time that Uber and Lyft start sharing our data,” said San Francisco driver Erica Mighetto. “So we can survive. This has really become a situation of survival—eating!”
If California drivers need money now, they could apply for unemployment as contractors and get it from the Coronavirus Aid, Relief and Economic Security (CARES) Act. But, in applying for that aid, they’d have to confirm their misclassification as contractors. And drivers want Uber and Lyft to pay them—not taxpayers.
Mighetto said she may have to file for the newly passed federal pandemic unemployment insurance as an independent contractor, even if she believes that’s not her employment status, because she needs the money.
But drivers worry that would set the wrong precedent. To avoid it, driver Tammie Jean Lane said she spent “hours” putting together a spreadsheet to prove her income, even though the companies could’ve shared it easily. “It shouldn’t be on us drivers when it’s something they should be doing,” she said.
As she tracked her wages, she did notice something though. She wasn’t crazy to think the mysterious algorithimic pay model didn’t always benefit her: She found a ride that cost the rider $138; she got about $60 of it.
“They call us independent contractors, they know that’s a lie,” said Frazier.
He said the coronavirus has exposed how the companies and its users treat drivers inhumanely.
Frazier remembered when he wanted to stop driving. A passenger—coughing and sneezing—from the Los Angeles airport got into his vehicle and said he “snuck in from Italy.” It was before the virus was widespread. But Frazier had a medical mask from the California fires he quickly put on.
“Me and the guy almost got into it,” Frazier remembers. “He said, ‘If you didn’t want to put your life on the line why would you even be doing a job like this?'”
Some of the housemates on 'Terrace House: Tokyo 2019–2020'.Netflix
An occasional series about stuff that’s getting us through a pandemic. More here.
An episode of Netflix’s Japanese reality show Terrace House goes something like this: Ruka gets home from working at a clothing store in Tokyo. He’s greeted by Haruka, who’s cooking ramen on the stove, and soon they’re eating dinner with four housemates who round out the show’s small cast. Like a little brother, Kaori and Haruka tease Ruka for not having decided on a career. They brainstorm ideas based on his passions, then the girls retreat upstairs to thoughtfully discuss their feelings. Risako isn’t sure how to respond to Kenji’s advances. She needs time to get to know him better. As she bites her lip, a pop song crescendoes. This is the Terrace House version of a cliffhanger.
Known as “the reality show where nothing happens,” TerraceHouse, which released new episodes of its Tokyo 2019-2020 installment last week, is my antidote for a time when too much is happening all at once. Kick back and soak in idyllic scenes from the year 2020 B.C. (Before Corona), when we left the house, sipped boba in parks, and entertained visitors with reckless abandon. The show centers the friendships, crushes, and romances that slowly develop among six housemates, with a level of nuance rarely seen in reality TV. But beyond the narcotic quality of its muted color palette and drama-free plot, Terrace House has brought me something deeper: a reminder that another world is possible.
When the US first came down with the ‘rona, I found strange comfort in watching Tiger King, not despite but because of its insanity. Friends and family joined me in drowning our troubles in the wild machinations of Joe Exotic and Carole Baskin, as memes about them infected our group chats in a manner that could only be called “viral.” The show’s addictive drama gave us something new to talk about: She totally killed her husband, but did she feed him to the tigers? As our president shrugged off the impending tsunami of death and collapse, Tiger King presented us with an alternate train-wreck, one that was actually possible to enjoy. Our national crisis remains uncertain and unending, but the show Doreen St. Félix summed up as “what we watched two weeks into our isolation” concluded after seven densely packed episodes, offering some bizarro form of surrogate catharsis.
It was hardly the first time I found guilty pleasure in a grotesque spectacle. From KFC’s decadent Double Down sandwich to Britney Spears’ sad, sedated dancing at the 2007 VMAs, I’ve long delighted in the “so bad it’s good.” Yet as our reality show president’s body count rises and the spectacle of his gaffes evolves from grotesque to scary, it feels as if there’s enough “bad” afoot to finally seek comfort in the actually comforting. In isolation, I newly appreciate the simple pleasures of being with others, of getting ready with girlfriends on a Saturday night, of the slow burn of a simmering crush who I’m not sure when I’ll see next. Terrace House frames such moments as if they were works of art.
What the show lacks in plot twists it makes up for in taste. Establishing shots are at once oblique and evocative, like video haiku: a train rolling through some trendy part of Tokyo; the full moon cresting a dew-speckled bush; steam rising off a mouth-watering dish before two castmates on a date dig in. Terrace House’s approach to reality TV is open-hearted and understated, with a focus on the familiar dynamics that arise when several people co-habitate. Pivotal scenes often involve one housemate calmly explaining to another how their actions have negatively affected the group, and that person pledging to do better. Every few episodes, someone’s in a sick mask because they have a cold, something Japanese people did to keep germs from spreading long before this plague. As strangers learning to live together, they prioritize the collective over the individual: the opposite of isolation.
So as Tiger King mania begins to fade, I invite you to join me in soothing your shellshock with this mundane yet fulfilling relic from the not-so-distant past. Your patience will pay off when Ruka finally gets his shit together, or when Risako decides, over a five-episode arc, that she’s into Kenji after all. Live vicariously through six people who have no idea what’s coming (and will be more prepared than us Americans when it does). Watching strangers slurp down ramen suddenly feels like medicine—or at least less like empty calories than what we’re usually binging.
A new study in Science Magazine about the transmission of the coronavirus sparked a wave of alarmingheadlines Wednesday declaring that social distancing mandates may have to remain in place into 2022. But the reality may not actually be so grim: The researchers’ model does not account for other ways of beating back the virus, such as effective medication that could prevent infected people from needing hospitalization, or even a vaccine.
A major focus of the effort to “flatten the curve” is to reduce the strain on the health care system. The new study, conducted by a team of researchers at the Harvard T.H. Chan School of Public Health, finds that under current critical care capacities, the pandemic could stretch into 2022. But, the authors write, “Increasing critical care capacity allowed population immunity to be accumulated more rapidly, reducing the overall duration of the epidemic and the total length of social distancing measures.” In other words, the more hospital beds, ventilators, and medical personnel we have to fight the virus, the less time we may be forced to spend cooped up in our homes.
And there are other steps the scientific community can take to stop the spread of the virus. “New therapeutics, vaccines, or other interventions such as aggressive contact tracing and quarantine—impractical now in many places but more practical once case numbers have been reduced and testing scaled up—could alleviate the need for stringent social distancing to maintain control of the epidemic,” the authors of the study write.
The study also assumes that the average number of people infected by someone with the virus is between 2 and 2.5. The number may actually be higher than that, which, MIT Technology Review points out, would be a good thing: If mild cases of the virus are more prevalent than we’d thought, herd immunity would be possible sooner.
In any event, social distancing will most likely not be a continuous reality over the next two years. The authors of the study envision intermittent phases of social distancing tailored to the prevalence of outbreaks and the preparedness of health care systems in specific communities.
“Keeping in mind that our goal is getting up to population-level immunity, in the absence of a vaccine or potentially other types of interventions, what we might see is this kind of on-off, intermittent distancing,” Yonatan Grad, one of the paper’s authors, told CNN. “And to get up to population immunity—again, that end point—would take until 2022.”
California will be the first state to provide financial assistance to undocumented immigrants affected by the coronavirus pandemic, in what advocates are calling a “necessary first step” to prevent families from falling deeper into a crippling financial crisis.
In a press conference Wednesday, Gov. Gavin Newsom announced the creation of the Disaster Relief Fund, which will give approximately 150,000 undocumented adults in California a one-time cash payment of $500, with a $1,000 cap per household. The fund will draw on $75 million from the state government and an additional $50 million from Grantmakers Concerned with Immigrants and Refugees, a network of foundations focused on immigration issues.
“Regardless of your status, documented or undocumented, there are people in need, and this is a state that steps up always to support those in need,” Newsom said. “We feel a deep sense of gratitude for people who are in fear of deportation but are still addressing the essential needs of tens of millions of Californians.”
Undocumented workers—including the estimated 4.6 million of them who file income taxes every year—were left out of the $2 trillion federal stimulus package passed by Congress last month. They don’t qualify for unemployment benefits.
California has the largest undocumented population in the United States, according to Pew Research Center estimates. Half of all California children are born to a household that has at least one person who is undocumented, and about 10 percent of the total workforce in the state is undocumented, Newsom said.
“This is a recognition of the fact that immigrant families are essential to our state,” Angelica Salas, executive director for the Coalition for Human Immigrant Rights (CHIRLA), said in a statement. “Immigrants are one-third of the workers in California who are in the front lines fighting COVID-19 and their loved ones are hurting from this pandemic, yet the federal government has ignored them.”
The cash assistance will be dispersed through “a community-based model” of regional nonprofits that serve undocumented communities in the state. Newsom said people can apply for aid starting next month.
“Today’s announcement is a necessary first step to close the widening gap between immigrants and vital assistance that could mean the difference between life and death for millions of Californians,” said Pablo Alvarado, co-director of the National Day Laborer Organization Network. “Our hope is that the actions taken by Gov. Newsom today will catalyze public and private partnerships to encourage additional measures to ensure that all people in California—regardless of immigration status—receive equal protection under the law.”
There’s a pandemic sweeping the globe that has already infected more than 2 million people and killed nearly 140,000. Three out of four people on Earth are under some form of lockdown in order to curb the spread of COVID-19, the illness caused by a novel coronavirus that first emerged last December in China. While epidemiologists, data scientists, and other public health experts struggle to understand the new virus and inform the public, another epidemic is spreading quickly: White guys on social media who suddenly have become infectious disease experts.
How many people will get sick? When will we be able to go out again? A vaccine is going to take how long? These are just a sampling of the questions we hope the specialists will answer. But that guy you went to high school with who has no relevant knowledge much less graduate degrees thinks you should listen to him instead.
Sure, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, has been doing this for 36 years, but that guy you vaguely know from summer camp just doesn’t think Fauci understands the disease like he does. “When this is all over, the country will know that Dr. Anthony Fauci was the anti-hero,” a Twitter user who self-identified as a retired math teacher but neglected to mention he doesn’t understand the meaning of “anti-hero” tweeted. “So wrong on number of deaths. Not one bit concerned about Americans and their loss of jobs.”
This outbreak of ill-placed expertise is not unique to the pandemic. In fact, the phenomenon of people with little knowledge acting as if they should be listened to has been studied and has some robust research behind it. They are all living, tweeting, opining, over-sharing examples of the Dunning-Kruger effect, a cognitive bias described back in 1999 by social psychologists David Dunning and Justin Kruger that explains why people overestimate their knowledge and abilities. A fine example is the president of the United States, who bragged about having an uncle who attended MIT and claimed that doctors kept asking him why he understood so much about the novel disease. “Maybe I have a natural ability,” President Donald Trump told reporters during a press conference at the CDC. “Maybe I should have done that instead of running for President.”
This combination of arrogance and stupidity also has been rampant among the armchair epidemiologists who have now emerged. Alex Berenson, former New York Times reporter turned right-wing media darling, said on Fox News that no one under 30 years old is at “serious risk” of this virus. That is simplynottrue.
Mark Humphries, an Australian comedian, captured what is going on perfectly in a video he tweeted on the topic. “My name is Dougall Merton and I’m a certified armchair epidemiologist. I graduated from the University of Wikipedia,” he says in the hilarious but painfully accurate satirical video. “It was only after a few days after graduation that I published my first peer-reviewed text message to friends and family.”
The armchair epidemiologist is everywhere and spans across age, race, and political leanings, but skews white and male. Because I’m extremely privileged to be healthy and safe at home, and because I’m a glutton for punishment, I mindlessly scroll through Facebook a few times a day.
Jaap Arriens/Zuma
One day, a friend of mine had posted an article warning about the dangers of misinformation during a public health crisis. Listen to the experts who want you to wash your hands and not your uncle’s wife who thinks the virus is caused by 5G cell phone towers. Simple, right? The first comment was from a man. “I think even the experts are misinformed.” Stunning! The World Health Organization, the Centers for Disease Control and Prevention, and the National Institute for Health, all got it wrong. But thank God, Chad from homeroom in 2005 has got a handle on the crisis.
Who are you going to listen to? The epidemiologists and data scientists or the guy who sat behind you in homeroom 15 years ago?
Soon the self-proclaimed experts started appearing up and down my feed. Another man commented on a different article about the science behind the models that try to figure out how many people will die from the virus. “I’m no medical expert,” he began, at which point he should have stopped. If you are not a medical expert, why are you offering your opinion on a medical topic? He did, of course, and went on to explain how long he thought it would be before infection rates would finally begin to slow.
And it’s not just Facebook. I’ve seen long Twitter threads opining about important aspects of the virus only to click on the user’s profile to find out it’s just some guy frustrated at home who, instead of taking care of his children, is just tweeting his hunches. The armchair experts are also posting screeds on Medium.com calling the virus a hoax or media-created hysteria. An infamous one by Silicon Valley technologist Aaron Ginn titled “Evidence Over hysteria—COVID-19” received millions of views before it was removed and reposted to a right-wing site. (With the death toll in the US quickly approaching 30,000, I’m sure their posts have aged quite nicely.) Even journalism outlets, who should just be telling the public what the experts are saying, have been guilty of this.
Before you start writing that hate e-mail that I will most definitely laugh at and then delete, I’m not singling out men unfairly; there’s some science—remember that?— to back me up. In the academic world, experts must cite their claims while writing a research paper. And, if you’re writing about an obscure topic with few experts, it’s not uncommon to cite yourself. In essence, you can be your own expert. In 2016, Molly King, a sociologist at Santa Clara University and several other researchers examined 1.5 million research papers between 1779 and 2011 and found that men cited themselves 56 percent more often than did women. In the last 20 years of their data, men cited themselves 70 percent more often than women cited themselves. King and the other researchers explain the wide gap in academic self-citations plainly: Men often tend to have inflated opinions of themselves and often face little backlash for overconfidence.
In fairness to the men in our social media feeds, the federal government’s utter failure in crafting a clear and effective response, crucial weeks spent dithering and denying, President Trump’s refusal to behave with clarity, consistency, or constructive leadership, and the states’ patchwork response, have left people without an essential, credible source of direction and information. So, it’s understandable that everyone across the country is trying to figure what we’re supposed to be doing, and what the end game looks like. But that’s where the public health experts come in. Not the random guy you forgot to unfriend a decade ago.
Kellie Burns spent much of last week asking urgent and personal questions of total strangers. Sitting cross-legged on her bed in Baltimore, in text after Facebook message after phone call, she pressed: When did you test positive for COVID-19? How long have you been feeling better?
Kellie wasn’t trying to socialize. She was just trying to save her father’s life.
Bill Burns was admitted two weeks ago, on Tuesday, March 31, to the intensive care unit at the Glens Falls Hospital in upstate New York, where he tested positive for the coronavirus. Bill, 62, had struggled with respiratory problems ever since working as a steamfitter on the post-9/11 Ground Zero cleanup.On Wednesday, he was put on a ventilator. On Thursday, Kellie asked her father’s doctors to get him a transfusion of convalescent plasma. Kellie, a former health care consultant who’d been tuning into New York Gov. Andrew Cuomo’s daily coronavirus briefings, had determined that the experimental treatment was the least risky, most feasible option to give her father a fighting chance.
Plasma therapy is a century-old medical practice that involves transferring the antibody-rich part of the blood, a yellowish liquid called plasma, from people who have recovered from a disease into those struggling to fight it off. It was used in the early 1900s to treat measles and mumps, and, more recently, to treat other coronaviruses, like MERS and SARS. Early outcomes from patients in China suggest that it could serve as a treatment for COVID-19, though, as Dr. Arturo Casadevall, an infectious diseases expert at Johns Hopkins University, explained, the “coronavirus is a new virus, and whenever you’re dealing with a new entity, you need testing.” In early April, the Food and Drug Administration unveiled a national study to test those interested in receiving the experimental treatment. Under the best-case scenario, plasma could treat sick patients while a longer-term therapy, like a vaccine, is developed.
Of the treatment options floating around in the news, plasma is the only therapy that has been used for decades and is known to be relatively safe, says Casadevall. Plus, it can be implemented quickly because it doesn’t require any drug development: Theoretically, the beneficial, virus-fighting antibodies exist in the blood of most people who have recovered from the coronavirus.
The problem is, “We don’t have an infrastructure for convalescent plasma,” says Casadevall. “It is being developed as we speak.”
In recent weeks, an alphabet soup of public health organizations, including the FDA, the Red Cross, and the American Association of Blood Banks (AABB), has come together in an attempt to quickly build a national plasma supply from scratch. The mobilization is unprecedented in scope, requiring the coordination of hundreds of hospitals and blood centers, and thousands of prospective donors and patients. But the process has been off to a clunky start, in part because there’s no clear person or group in charge. “People talk about the blood supply as though there’s a single national blood system, which there isn’t,” said Eduardo Nunes, the AABB’s vice president of quality and standards. “There isn’t a single, centralized point of decision making to the entire community.”
For now, the plasma supply is minuscule: Plasma needs to come from people who tested positive for the coronavirus and haven’t exhibited symptoms for weeks, in addition to meeting the typical criteria for blood donation, like having enough iron and not being on certain medications. Blood banks across the country are in the early stages of soliciting donors. “It’s very frustrating for me to have to tell people, ‘I’m sorry, but we don’t have it yet,’” said Dr. Louis Katz, the acting chief medical officer at Mississippi Valley Regional Blood Center, which has locations across the Midwest. “We’re building an airplane as we fly.”
As a result, families like Kellie’s are left with few options. Some are starting to plead with medical professionals—on Thursday, Katz received phone calls from three doctors representing desperate families in just the 20 minutes before we talked—while others are turning to social media and local news outlets in search of donors for their loved ones. Survivor Corps, a Facebook group with more than 30,000 members, functions as part support group for COVID-19 patients and their families and part grassroots plasma donor network, with pleas from family members across the country looking for donors and specifying the blood type they’re looking for. The messages are equal parts devastating and inspiring. “My husband is currently fighting for his life, on a ventilator, in the ICU,” read one post on Sunday. “Please help if you are able. This disease is nasty and terrifying.”
On Tuesday, another woman wrote, “Hey my doctor just called and said I am free of covid!!!” She continued, “Now how can I go and donate my plasma in Los Angeles. Anyone know? I would love to help as many people as I can.”
Glens Falls is a small hospital, and Bill Burns was among the first coronavirus patients admitted to its ICU. When Kellie first spoke with his doctors and nurses over the phone from her home in Baltimore—like other hospitals, Glens Falls has shut down access to visitors—she felt the staff weren’t responsive to her pleas. “They’re frantically trying to figure out what the best things are, too,” she told me.
So Kellie took matters into her own hands. She started reading up on the FDA process for getting plasma from donor to patient. On Saturday, April 4, Kellie finally connected on the phone with hospital staffers who had a moment to spare, who then contacted the FDA and the American Red Cross about getting plasma for Bill. An email from the American Red Cross to Bill’s pulmonologist explained that the organization was in the process of building up a plasma inventory, but things were still very preliminary. In the meantime, it read, “We need the hospitals’ assistance to find an appropriate donor.”
In other words, if Bill was going to get plasma, someone else was going to have to find it.
Kellie knew that plasma was no panacea. “What’s weird about this is, you’re fighting hard for something that could have no effect,” she told me last week. “All you can do in this situation is make sure you don’t have any regrets about how you tried to help your loved one.”
Bill Burns with Kellie’s daughter, Hazel
Kellie Burns
On Sunday, Kellie took to Facebook: “Our father is still in critical condition with COVID-19 and after speaking with his doctor, we believe that plasma from a recovered patient is his next best treatment option. The problem is, WE NEED A DONOR!” The post was shared nearly 300 times in three days, and Kellie started getting texts, calls, and emails from strangers who wanted to help—so many that Kellie and her five siblings were having trouble keeping up. On lively family video chats—“I’m from very loud, big Italian family,” Kellie explained—they shared regular status reports from the hospital and donor leads.
According to FDA’s rules, donors have to be symptom-free for at least two weeks and test negative for the coronavirus, or be asymptomatic for at least four weeks. (Eventually, prospective donors may have to take antibody tests, but for now, the accessibility and accuracy of such tests are too limited.) Some of the people Kellie talked to had been diagnosed with the coronavirus by a doctor but never got the official positive test. Others had trouble getting the second test to show they were negative. Given the short supply of diagnostic tests, it seemed virtually impossible to know who had viable plasma, particularly if they were under the 28-day mark. “That is one of the big stumbling blocks at the moment to opening the taps as wide as we possibly can,” said Dr. Claudia Cohn, chief medical officer of AABB.
People whom Kellie had never met before went to extreme lengths to help. One complete stranger in Chicago offered to get on a plane and fly to Albany to donate her plasma for Bill. Another drove from New Jersey to Manhattan during his lunch break after Kellie learned that the New York Health Department would be testing some ConEd workers for the coronavirus that afternoon and had one extra test to spare. A third prospective donor, a nurse in Glens Falls named Tony, drove three hours to Syracuse to get tested.
“It’s unbelievable how kind people have been, how much they want to help,” Kellie said.
But five days after her call for plasma, after being glued to her phone while her husband took care of their 15-month-old daughter, Kellie was still out of luck. “Long story short, we don’t yet have a qualified donor,” she wrote on Facebook on Friday, April 10. “We had 3 very promising candidates as of this morning, but by 8pm all 3 had been disqualified.” One didn’t have the right kind of testing; the other two had once again tested positive. Her father was still alone in the ICU, sedated on a breathing tube, and running out of time.
Meanwhile, Kellie was noticing more and more petitions on social media asking for plasma. “It’s getting to the point where you see it and you’re like, this is just silly,” she told me. “It can’t be this way—where people are looking for individual donors.”
It’s not supposed to be this way. In theory, any hospital that is enrolled in the FDA’s new Expanded Access study, which is run by the Mayo Clinic, will soon have access to an inventory of plasma available at local blood centers—a process similar to how blood is managed. That way, people like Kellie won’t have to solicit direct donations, and the system won’t give preference to families who have the resources to advocate for themselves.
Usually, hospitals have to work through layers of red tape to participate in federal investigative studies, but the FDA waived many of the usual rules to fast track the plasma donation process: Hospitals and doctors interested in plasma transfusion simply fill out a few online forms. Glens Falls Hospital enrolled in the study last week, on Bill’s ninth day on the ventilator. Since the registration website went live 12 days ago, more than 1,000 hospital sites have signed up to participate.
A steady supply of plasma is likely weeks away, experts say. As of Tuesday, 118 patients had received plasma transfusions through the Mayo Clinic study. The American Red Cross collected plasma from just five donors last week, producing 15 units of convalescent plasma, each of which can help one person. In hard-hit New York, hundreds of donation registrations have come into New York Blood Center since Gov. Cuomo encouraged coronavirus survivors to donate plasma during his press conference last week. But as of Friday, the center, which was among the first in the country to get a donation program up and running, and which provides nearly all the blood to hospitals in New York City and the Hudson Valley, only had enough plasma to reserve two units per hospital. New Yorkers will “certainly be the source of a lot of plasma in coming weeks and months” as other regions hit their peaks, said Katz. “It’s unfortunate that we can’t just turn on the spigot, but it’s also true.”
In the weeks to come, while plasma demand outpaces supply, blood banks, hospitals, doctors across the nation will face thorny questions: Who deserves this experimental treatment? If a patient’s family finds a donor for their loved one, should that donation actually be directed to the patient? What happens to the many families who don’t have the time or resources to take to Facebook and reach out to local news channels? Then, there’s the question of severity: Evidence suggests that those who are earlier along in the disease will benefit more from plasma than those who have progressed and are much sicker, says Cohn. But “ethically, you feel like they deserve every treatment that’s available,” she says. “That’s going to be a very difficult call to make. The collective hope is to get to a point where the supply where we’re no longer dealing with this.”
Katz, for one, told me on Thursday that since going live with its convalescent plasma collection last week, the Mississippi Valley Blood Center had so far identified one potentially eligible donor. I asked how he was going to decide which three lucky patients would receive it. He groaned, said, “Oh, Lord,” and added, “I think it’s going to be first come, first serve. I mean, am I supposed to decide who’s too sick and not sick enough? I don’t think that I’m qualified to do that—or anybody else is.”
On Saturday evening, during a group FaceTime with her family, Kellie got a call from the hospital. It was her father’s doctor. She got straight to the point: “Your dad is about to get the plasma transfusion.”
While Kellie had been pleading with strangers, the system worked as it was supposed to: A recovered coronavirus patient in Long Island donated plasma to New York Blood Center’s nascent inventory, and Glens Falls Hospital, equipped with its FDA study enrollment, had put in a request for plasma. Miraculously, Bill Burns got one of the few doses in stock. On Saturday afternoon, a courier drove the blood three hours from Long Island to Glens Falls.
“WE DID IT!!!” Kellie wrote on Facebook on Saturday evening. “Thank you to every single person (and there were many!) who made this a reality. It was totally unexpected and it didn’t happen the way we thought it would, but it happened. I will definitely share more details later, but for now I am going to sleep!”
When I spoke to Kellie on Sunday, the high had worn off a bit. If the plasma transfusion works, it will likely take two to three days to show any effect, leaving the Burns family in an anguished waiting game.
The Burns family during Christmas of 2019
Kellie Burns
On Sunday, they learned that Bill had developed a bacterial infection, which is common for patients intubated for long periods of time. By that point, the Burns family hadn’t laid eyes on Bill for 12 days, and the nurses offered to hold up an iPad so the family could talk to him. On the screen, Bill had a tube hanging out of his mouth. The drugs had stilled him. Kellie could almost pretend that he was just sleeping. The faces of the Burns kids and their mother filled the screen, but no one knew quite what to say. Kellie’s mother tearfully said “I love you” over and over, adding that their two dogs missed Bill, too. Bill is a big sports guy—he’d coached his sons’ football teams—and on the phone, the now-grown sons told their father to keep up the fight.
The call lasted just four minutes. “There’s only so much you can say, right?” Kellie told me afterwards, sounding exhausted. “You’re just hoping that they hear your voice. Even that just feels enormous at this point.”
Those who are interested in donating plasma can find more information on the AABB website.
In the absence of a vaccine, enough ventilators to contain the coronavirus, or a president capable of putting the country’s needs ahead of his own, it’s tempting to dismiss Trump’s press conferences as the propaganda pageants they are—and back slowly away from his Twitter account, a feedingground for the world’s largest ego.
Can we? Mute @realDonaldTrump for a minute? No. We’d miss too many high-impact statements that have consequences in our lives, whether we cringe at his tweets or not, from a president who one conservative New York Times columnist charitably calls a “sociopath,” a designation more and moreexpertsaremaking.
Even if you’re not in the diagnosis business, I do wonder if this country’s spirits wouldn’t be lifted by watching Trump undergo a devastating brush with something more consequential, ruthless, and upending than anything else: a copy edit.
Here, in the name of national security and public hygiene, is an emergency deployment of the finest tool Mother Jones has available: the annotation feature. Click on the highlights below, like this, to instantly improve the president’s tweets and our country’s health.
96-0 in the United States Senate. Congratulations AMERICA!
96-0 in the United States Senate. Congratulations AMERICA!
"My Administration is actively planning the next phase in an all-out war against this horrible virus." pic.twitter.com/pqejbUifTc
— The White House 45 Archived (@WhiteHouse45) March 27, 2020
“My Administration is actively planning the next phase in an all-out war against this horrible virus.”
I love Michigan, one of the reasons we are doing such a GREAT job for them during this horrible Pandemic. Yet your Governor, Gretchen “Half” Whitmer is way in over her head, she doesn’t have a clue. Likes blaming everyone for her own ineptitude! #MAGA
I love Michigan, one of the reasons we are doing such a GREAT job for them during this horrible Pandemic. Yet your Governor, Gretchen “Half”Whitmer is way in over her head, she doesn’t have a clue. Likes blaming everyone for her own ineptitude! #MAGA
I just signed the CARES Act, the single biggest economic relief package in American History – twice as large as any relief bill ever enacted. At $2.2 Trillion Dollars, this bill will deliver urgently-needed relief for our nation’s families, workers, and businesses. #CARESAct🇺🇸 https://t.co/0WnTNFZPZD
I just signed the CARES Act, the single biggest economic relief package in American History – twice as large as any relief bill ever enacted. At $2.2 Trillion Dollars, this bill will deliver urgently-needed relief for our nation’s families, workers, and businesses. #CARESAct🇺🇸
General Motors MUST immediately open their stupidly abandoned Lordstown plant in Ohio, or some other plant, and START MAKING VENTILATORS, NOW!!!!!! FORD, GET GOING ON VENTILATORS, FAST!!!!!! @GeneralMotors@Ford
General Motors MUST immediately open their stupidly abandoned Lordstown plant in Ohio, or some other plant, and START MAKING VENTILATORS, NOW!!!!!! FORD, GET GOING ON VENTILATORS, FAST!!!!!! @GeneralMotors @Ford
….I have been packed all day with meetings, I have no time for stupidity. We’re working around the clock to KEEP AMERICA SAFE!
On the recommendation of the White House CoronaVirus Task Force, and upon consultation with the Governor’s of New York, New Jersey and Connecticut, I have asked the @CDCgov to issue a strong Travel Advisory, to be administered by the Governors, in consultation with the….
On the recommendation of the White House CoronaVirus Task Force, and upon consultation with the Governor’s of New York, New Jersey and Connecticut, I have asked the @CDCgov to issue a strong Travel Advisory, to be administered by the Governors, in consultation with the….
For the purpose of creating conflict and confusion, some in the Fake News Media are saying that it is the Governors decision to open up the states, not that of the President of the United States & the Federal Government. Let it be fully understood that this is incorrect….
For the purpose of creating conflict and confusion, some in the Fake News Media are saying that it is the Governors decision to open up the states, not that of the President of the United States & the Federal Government. Let it be fully understood that this is incorrect….
If the Fake News Opposition Party is pushing, with all their might, the fact that President Trump “ignored early warnings about the threat,” then why did Media & Dems viciously criticize me when I instituted a Travel Ban on China? They said “early & not necessary.” Corrupt Media!
If the Fake News Opposition Party is pushing, with all their might, the fact that President Trump “ignored early warnings about the threat,” then why did Media & Dems viciously criticize me when I instituted a Travel Ban on China? They said “early & not necessary.” Corrupt Media!
The Lamestream Media wants us to fail. That will NEVER happen!
If additional literature from @realDonaldTrump needs a constitutional touch-up, send it to styleguide@motherjones.com and we’ll update this post with a few of the finest. #MAGAZINE 🇺🇸
President Donald J. Trump delivers remarks during a news conference in the Rose Garden of the White House in Washington D.C., U.S. on Tuesday, April 14, 2020.
Stefani Reynolds/CNP via ZUMA Wire
In a bizarre press conference on Tuesday, President Donald Trump faulted the World Health Organization for an error that he himself has been slammed for making.
In a move that Trump previewed last week was in the works, the president said he is imposing a freeze on US funding to the WHO “while a review is conducted to assess” the organization’s role in “severely mismanaging and covering up the spread of the coronavirus. Everybody knows what is going on there.”
Trump went on to fault the WHO for opposing his February 2 restriction on travel from China—a step he has ceaselessly touted as life saving, despite it coming after around 400,000 people traveled from China to the US and the fact that it’s failed to prevent an additional 40,000 from coming since. Trump also assailed the organization for passing on inaccurate information about the outbreak from China. “The WHO failed to investigate credible reports from sources in Wuhan that conflicted directly with the Chinese government’s official accounts,” Trump said.
Left out of this account is reality. According to multiplereports, US officials did not believe the Chinese efforts to downplay the severity of the outbreak in Wuhan and, beginning in January, warned the president the virus would have a severe impact on the US. Trump, however, dismissed these warnings, in part because he apparently accepted assurances from Chinese President Xi Jinping.
The Washington Postreported on March 20 that when his advisers warned that he would have to promote economically disruptive measures to combat the virus, Trump’s “insistence on the contrary seemed to rest in his relationship with China’s President Xi Jinping, whom Trump believed was providing him with reliable information about how the virus was spreading in China, despite reports from intelligence agencies that Chinese officials were not being candid about the true scale of the crisis.”
When advisers told Trump “that Beijing was not providing accurate numbers of people who were infected or who had died,” the Post noted, Trump ignored them and publicly praised China on his favorite medium:
China has been working very hard to contain the Coronavirus. The United States greatly appreciates their efforts and transparency. It will all work out well. In particular, on behalf of the American People, I want to thank President Xi!
Despite this, or perhaps because of it, Trump on Tuesday attacked the WHO for “praising China for its so-called transparency”—note that’s the same word he himself used. Later in the presser, the president angrily brushed off reporters’ questions about this contradiction, responding with non-sequiturs.
With Trump’s effort to scapegoat the WHO, it’s important to note that the president lacks legal power to freeze money already appropriated by Congress—a fact highlighted in a January GAO report that found Trump’s hold last year on congressionally approved aid to Ukraine, which factored in his impeachment, was illegal. “The President DOES NOT have the authority to permanently withhold funds lawfully appropriated by Congress,” Rep. Don Beyer (D-Va.) tweeted. “You might think Donald Trump would have learned this important fact during the past 9 months!”
Trump’s attacks on the WHO were just one part of an incredibly over-the-top press performance on Tuesday. The presser, held in White House Rose Garden, began more an hour late. After attacking the WHO, and without mentioning the more than 25,000 Americans already killed by the coronavirus, Trump struck a tone of self-congratulation, thanking a long-list of CEOs for undetermined actions.
"Pepsi Cola, Chick-fil-A, Subway, Yum Brands, Papa John's" — Trump is still reading off the names of random companies during a press briefing that is ostensibly about a deadly pandemic that is killing Americans pic.twitter.com/NgsiIWX6KD
Pressed by reporters on the unavailability of coronavirus tests, Trump attempted a tough tone, vowing to hold governors “accountable” for shortfalls in tests and protective equipment widely seen as a federal responsibility. (Don’t forget Trump falsely claimed on March 7 that “anyone who wants a test can get a test.”) This claim that governors are responsible for testing came one day after Trump used the daily coronavirus task force briefing to assert his dominance over governors, insisting that as president he has total authority to reopen businesses, schools, and other key points of life in individual states.
Dr. Anthony Fauci, speaks as President Donald Trump listens on April 10, 2020.Kevin Dietsch/CNP via ZUMA Wire
President Trump said Monday evening that he will not fire Dr. Anthony Fauci, head of the National Institute of Allergy and Infectious Diseases and the administration’s most trusted voice on the coronavirus pandemic—a reassurance that became necessary after Trump on Sunday retweeted a call to “#FireFauci.”
But could Trump actually fire Fauci if he wanted to? It’s not so simple. Even if you put aside the political firestorm it would cause, Trump could not just oust Fauci from his position by tweet. He would need to tell Fauci’s supervisor to remove him, and that person would need to state a valid cause in writing, with the outcome subject to a legal appeal, according to federal employment law experts I surveyed.
To be sure, Trump could easily remove Fauci from his position on the coronavirus task force and his role in televised briefings. That is one possible course of action that some right-wingers are urging Trump to take to punish the doctor for various perceived sins, such as admitting on CNN Sunday the patently obvious fact that a quicker government response to the crisis “could have saved lives.” (Fauci said Monday that he did not intend to suggest that Trump had caused deaths by failing to act faster.) The president also has the means to try to cause Fauci’s resignation.
But assuming that those telling Trump to “fire Fauci” mean literally removing him from the NIAID job Fauci has held since 1984, it’s important to note: The president cannot do that with just a snap of his fingers. Trump said Monday that as president, his “authority is total.” It is not. Trump was talking about ordering states to “reopen” after their coronavirus-related shutdowns, a power that the Constitution likely denies him. But another limitation on his authority comes from federal workplace laws that restrict the president’s power to dismiss officials like Fauci over a perceived lack of political loyalty.
Fauci, according to the NIAID, is a “Title 42” employee. That’s a special federal employment category for scientists and specialized consultants who work mostly in the Health and Human Services Department or the Environmental Protection Agency. While they don’t have normal civil service protections, they can only be fired through a specific process.
“There would have to be cause,” said William Wiley, a former chief counsel to the chair of the Merit Systems Protection Board, a quasi-judicial federal agency that hears federal employment disputes. “He would have to be fired for a valid reason.” Wiley said such a firing would have to be done in writing and that Fauci could appeal a dismissal as invalid. “If they want to remove him from employment they have to tell him why and give him a chance to defend himself,” Wiley said.
Such a firing would have to be for one of two basic reasons, Wiley said: poor performance or refusal to comply with rules or orders. There is also some precedent for firing a federal official for actions they weren’t explicitly told to avoid, but which the official should have known his or her boss would object to. The White House could argue such a standard permitted removing Fauci for statements like those he made on CNN, Wiley said.
Federal workplace law experts also noted that Trump himself can’t fire Fauci, who is not a presidential appointee. “President Trump probably cannot remove Dr. Fauci,” Debra Katz, a prominent federal whistleblower attorney, said via email. Katz said Trump would need to instruct one of Fauci’s nominal bosses, HHS Secretary Alex Azar or National Institutes of Health Director Francis Collins, to remove him. At least in theory, they could refuse.
Of course, there is no question that Fauci’s primary job security is political. Fauci is far more trusted than Trump, and the president, already damaged by his struggle to respond to the pandemic, could worsen the political hit by dismissing the much-admired Fauci. A recent Quinnipiac poll found that 78 percent of Americans approved of Fauci’s handling of the coronavirus, compared to 46 percent for Trump. Even among Trump supporters, Fauci is overwhelmingly trusted. Sixty-nine percent of Fox News watchers trust Fauci, compared to 14 percent who do not, a Navigator tracking poll released Monday found.
“What Fauci has going for him is his reputation, and his public viability for a long time under both Democratic and Republican presidents,” said Peter Shane, an Ohio State constitutional law professor who studies executive power.
But “Fauci is not going to live forever,” and eventually an official “who does not enjoy the reputation Fauci does” will have to tell a president hard truths about a public health emergency, Shane noted. That is why we have a system set up to give experts some protection against presidential whim.
The line for lunch at Sharing Caring Hands on Tuesday, March 24, in Minneapolis.David Joles/Star Tribune/AP
Food banks across the United States are struggling amid droves of hungry Americans in need of a meal. And images from photographers around the country show the horrifying number of Americans lining up to receive food assistance.
Anaheim, California: Cars were lined up about a half mile long in both directions of the 57 Freeway to get to Second Harvest Food Bank
Mindy Schauer/MediaNews Group/Orange County Register/Getty
“We’re looking at an increase of 17.1 million people over the course of the next six months,” Claire Babineaux-Fontenot, CEO of Feeding America, one of the country’s largest hunger-relief organizations, told NBC News. Babineaux-Fontenot highlighted a 98 percent increase in demand for free food and Feeding America, expects to lose $1.4 billion trying to survive.
Minneapolis, Minnesota: Cars line up at a drive-thru food pantry.
Neil Blake/Grand Rapids Press/AP
Des Moines, Iowa: Over 100,000 Iowans filed first time claims for unemployment in the last three weeks. People started lining up 3 hours before the food distribution began.
Jack Kurtz/ZUMA
In San Antonio, ten thousand cars waited at a food distribution point run by the San Antonio Food Bank. CEO Eric Cooper told NBC’s Hoda Kotb on the Today Show that the bank typically feeds about 60,000 people a week—it’s now about 120,000 people a week.
According to the Guardian, the number of people lining up in Phoenix, Arizona has tripled. Across southern Arizona, it doubled. In Las Vegas, where demand is up by 30 percent, one of the largest food pantries has shuttered 170 out of 180 locations. In Massachusetts, food pantries increased distribution by 849 percent.
Des Moines, Iowa: Maria Cunningham sorts bags of food before a drive through emergency food distribution at First DSM Church. DSM has increased their food pantry from one day weekly to three days per week.
Jack Kurtz/ZUMA
Detroit, Michigan: The Gleaners Community Food Bank distributes free food to residents in need in southwest Detroit.
Jim West/ZUMA
Sheila Christopher, director of Hunger-Free Pennsylvania, told the Guardian that she’s “been in this business over 30 years, and nothing compares to what we’re seeing now.” Jennifer McLean, the CEO of NYC’s City Harvest, told the New York Times that the need they’re seeing now dwarfs other crises like Hurricane Sandy and even September 11th.
People wait in their cars Thursday, at Traders Village for the San Antonio Food Bank to begin food distribution. 10,000 people seek San Antonio Food Bank help.
William Luther/San Antonio Express News/ZUMA
But as more Americans find themselves relying on these organizations, those running these programs are facing the pandemic too. Dependent on volunteers, food banks across the country are coming up short on labor while people hunker down. In places like Washington state and Louisiana the National Guard has been called in to help with labor shortages. The Washington Post reported that many volunteer shifts have been canceled, because much of the labor that food banks rely on is comprised of retirees and senior citizens. To top it all off, Feeding America reported that they’ve seen a 64 percent decrease in donations.
The images are almost apocalyptic, flashing by in the collage of pictures that populate the intro to a sci-fi film. They’re also becoming frighteningly common.
Sunrise, Florida: Feeding South Florida has seen a 600 percent increase in the those asking for food aid as people, some of whom have lost jobs, need to make ends meet during the coronavirus pandemic.
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
Billionaires own the media, but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what we deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.
Billionaires own the media, but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what we deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.